Download
1 / 1
10 likes | 179 Views
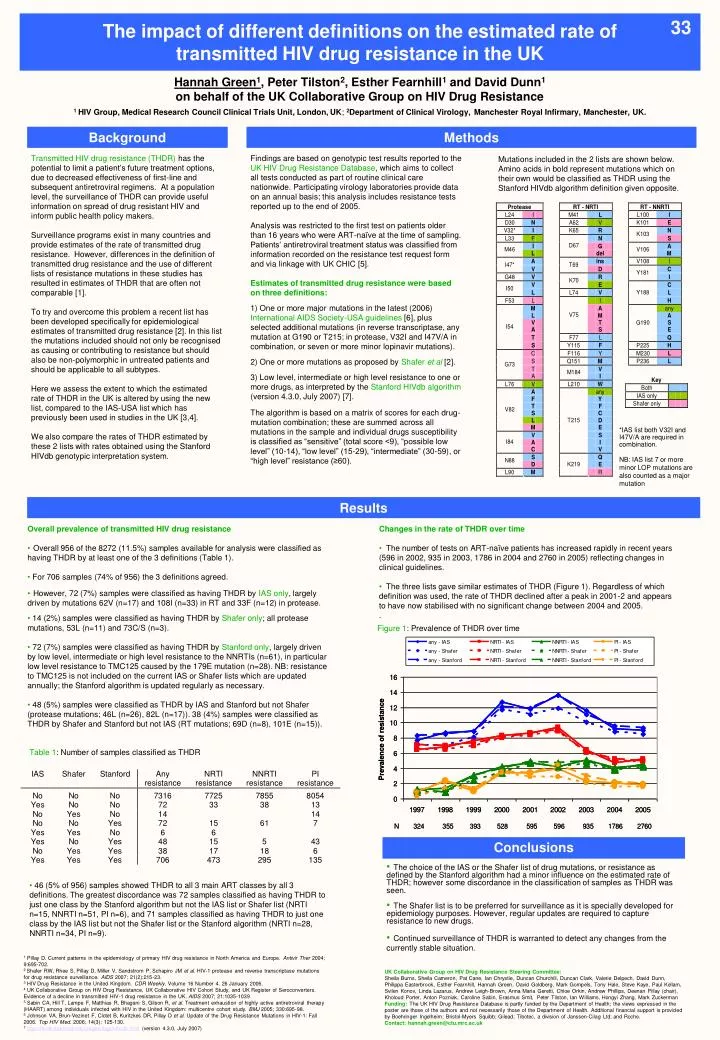
Table 1 : Number of samples classified as THDR. Conclusions. Background. Methods. Results. 33. The impact of different definitions on the estimated rate of transmitted HIV drug resistance in the UK. The UK HIV Drug Resistance Database: Development and use for national surveillance.

E N D
Table 1: Number of samples classified as THDR Conclusions Background Methods Results 33 The impact of different definitions on the estimated rate of transmitted HIV drug resistance in the UK The UK HIV Drug Resistance Database: Development and use for national surveillance Hannah Green1, Peter Tilston2, Esther Fearnhill1 and David Dunn1on behalf of the UK Collaborative Group on HIV Drug Resistance 1 HIV Group, Medical Research Council Clinical Trials Unit, London, UK; 2Department of Clinical Virology, Manchester Royal Infirmary, Manchester, UK. Transmitted HIV drug resistance (THDR) has the potential to limit a patient’s future treatment options, due to decreased effectiveness of first-line and subsequent antiretroviral regimens. At a population level, the surveillance of THDR can provide useful information on spread of drug resistant HIV and inform public health policy makers. Surveillance programs exist in many countries and provide estimates of the rate of transmitted drug resistance. However, differences in the definition of transmitted drug resistance and the use of different lists of resistance mutations in these studies has resulted in estimates of THDR that are often not comparable [1]. To try and overcome this problem a recent list has been developed specifically for epidemiological estimates of transmitted drug resistance [2]. In this list the mutations included should not only be recognised as causing or contributing to resistance but should also be non-polymorphic in untreated patients and should be applicable to all subtypes. Here we assess the extent to which the estimated rate of THDR in the UK is altered by using the new list, compared to the IAS-USA list which has previously been used in studies in the UK [3,4]. We also compare the rates of THDR estimated by these 2 lists with rates obtained using the Stanford HIVdb genotypic interpretation system. Findings are based on genotypic test results reported to the UK HIV Drug Resistance Database, which aims to collect all tests conducted as part of routine clinical care nationwide. Participating virology laboratories provide data on an annual basis; this analysis includes resistance tests reported up to the end of 2005. Analysis was restricted to the first test on patients older than 16 years who were ART-naïve at the time of sampling. Patients’ antiretroviral treatment status was classified from information recorded on the resistance test request form and via linkage with UK CHIC [5]. Estimates of transmitted drug resistance were based on three definitions: 1) One or more major mutations in the latest (2006) International AIDS Society-USA guidelines [6], plus selected additional mutations (in reverse transcriptase, any mutation at G190 or T215; in protease, V32I and I47V/A in combination, or seven or more minor lopinavir mutations). 2) One or more mutations as proposed by Shafer et al [2]. 3) Low level, intermediate or high level resistance to one or more drugs, as interpreted by the Stanford HIVdb algorithm (version 4.3.0, July 2007) [7]. The algorithm is based on a matrix of scores for each drug-mutation combination; these are summed across all mutations in the sample and individual drugs susceptibility is classified as “sensitive” (total score <9), “possible low level” (10-14), “low level” (15-29), “intermediate” (30-59), or “high level” resistance (≥60). Mutations included in the 2 lists are shown below. Amino acids in bold represent mutations which on their own would be classified as THDR using the Stanford HIVdb algorithm definition given opposite. *IAS list both V32I and I47V/A are required in combination. NB: IAS list 7 or more minor LOP mutations are also counted as a major mutation • Overall prevalence of transmitted HIV drug resistance • Overall 956 of the 8272 (11.5%) samples available for analysis were classified as having THDR by at least one of the 3 definitions (Table 1). • For 706 samples (74% of 956) the 3 definitions agreed. • However, 72 (7%) samples were classified as having THDR by IAS only, largely driven by mutations 62V (n=17) and 108I (n=33) in RT and 33F (n=12) in protease. • 14 (2%) samples were classified as having THDR by Shafer only; all protease mutations, 53L (n=11) and 73C/S (n=3). • 72 (7%) samples were classified as having THDR by Stanford only, largely driven by low level, intermediate or high level resistance to the NNRTIs (n=61), in particular low level resistance to TMC125 caused by the 179E mutation (n=28). NB: resistance to TMC125 is not included on the current IAS or Shafer lists which are updated annually; the Stanford algorithm is updated regularly as necessary. • 48 (5%) samples were classified as THDR by IAS and Stanford but not Shafer (protease mutations; 46L (n=26), 82L (n=17)). 38 (4%) samples were classified as THDR by Shafer and Stanford but not IAS (RT mutations; 69D (n=8), 101E (n=15)). • Changes in the rate of THDR over time • The number of tests on ART-naïve patients has increased rapidly in recent years (596 in 2002, 935 in 2003, 1786 in 2004 and 2760 in 2005) reflecting changes in clinical guidelines. • The three lists gave similar estimates of THDR (Figure 1). Regardless of which definition was used, the rate of THDR declined after a peak in 2001-2 and appears to have now stabilised with no significant change between 2004 and 2005. • . Figure 1: Prevalence of THDR over time • The choice of the IAS or the Shafer list of drug mutations, or resistance as defined by the Stanford algorithm had a minor influence on the estimated rate of THDR; however some discordance in the classification of samples as THDR was seen. • The Shafer list is to be preferred for surveillance as it is specially developed for epidemiology purposes. However, regular updates are required to capture resistance to new drugs. • Continued surveillance of THDR is warranted to detect any changes from the currently stable situation. • 46 (5% of 956) samples showed THDR to all 3 main ART classes by all 3 definitions. The greatest discordance was 72 samples classified as having THDR to just one class by the Stanford algorithm but not the IAS list or Shafer list (NRTI n=15, NNRTI n=51, PI n=6), and 71 samples classified as having THDR to just one class by the IAS list but not the Shafer list or the Stanford algorithm (NRTI n=28, NNRTI n=34, PI n=9). 1 Pillay D. Current patterns in the epidemiology of primary HIV drug resistance in North America and Europe. Antivir Ther 2004; 9:695-702. 2 Shafer RW, Rhee S, Pillay D, Miller V, Sandstrom P, Schapiro JM et al. HIV-1 protease and reverse transcriptase mutations for drug resistance surveillance. AIDS 2007; 21(2):215-23. 3 HIV Drug Resistance in the United Kingdom. CDR Weekly. Volume 16 Number 4. 26 January 2006. 4 UK Collaborative Group on HIV Drug Resistance, UK Collaborative HIV Cohort Study, and UK Register of Seroconverters. Evidence of a decline in transmitted HIV-1 drug resistance in the UK. AIDS 2007; 21:1035-1039 5 Sabin CA, Hill T, Lampe F, Matthias R, Bhagani S, Gilson R, et al. Treatment exhaustion of highly active antiretroviral therapy (HAART) among individuals infected with HIV in the United Kingdom: multicentre cohort study. BMJ 2005; 330:695-98. 6 Johnson VA, Brun-Vezinet F, Clotet B, Kuritzkes DR, Pillay D et al. Update of the Drug Resistance Mutations in HIV-1: Fall 2006. Top HIV Med. 2006; 14(3): 125-130. 7http://hivdb.stanford.edu/pages/algs/HIVdb.html (version 4.3.0, July 2007) UK Collaborative Group on HIV Drug Resistance Steering Committee: Sheila Burns, Sheila Cameron, Pat Cane, Ian Chrystie, Duncan Churchill, Duncan Clark, Valerie Delpech, David Dunn, Philippa Easterbrook, Esther Fearnhill, Hannah Green, David Goldberg, Mark Gompels, Tony Hale, Steve Kaye, Paul Kellam, Svilen Konov, Linda Lazarus, Andrew Leigh-Brown, Anna Maria Geretti, Chloe Orkin, Andrew Phillips, Deenan Pillay (chair), Kholoud Porter, Anton Pozniak, Caroline Sabin, Erasmus Smit, Peter Tilston, Ian Williams, Hongyi Zhang, Mark Zuckerman Funding: The UK HIV Drug Resistance Database is partly funded by the Department of Health; the views expressed in the poster are those of the authors and not necessarily those of the Department of Health. Additional financial support is provided by Boehringer Ingelheim;Bristol-Myers Squibb; Gilead; Tibotec, a division of Janssen-Cilag Ltd; and Roche. Contact: hannah.green@ctu.mrc.ac.uk