Download
1 / 1
10 likes | 218 Views
18 year old with NSTEMI: Anomalous Right Coronary Artery Mary Hendricks, MS, DO 1 Sarah Nease , MD 2 Steven Hollosi , DO 1 Charleston Area Medical Center, Department of Emergency Medicine 1 ; Charleston Area Medical Center, Department of Cardiology 2. INTRODUCTION

E N D
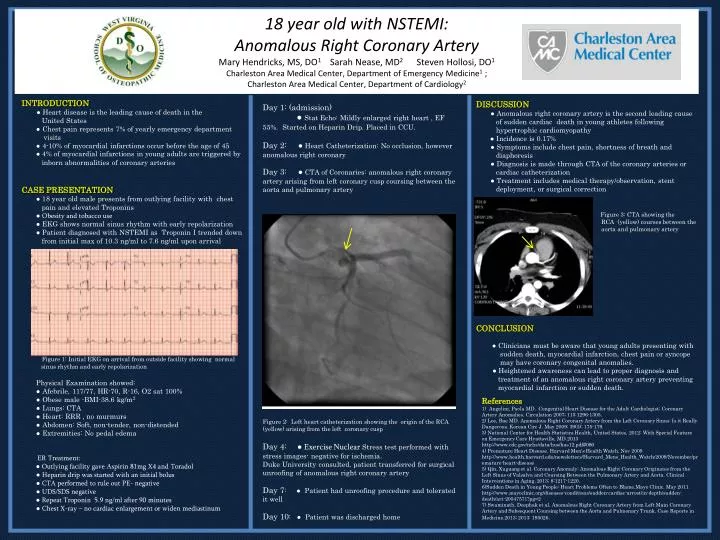
18 year old with NSTEMI: Anomalous Right Coronary Artery Mary Hendricks, MS, DO1 Sarah Nease, MD2 Steven Hollosi, DO1 Charleston Area Medical Center, Department of Emergency Medicine1 ; Charleston Area Medical Center, Department of Cardiology2 • INTRODUCTION • ● Heart disease is the leading cause of death in the • United States • ● Chest pain represents 7% of yearly emergency department • visits • ● 4-10% of myocardial infarctions occur before the age of 45 • ● 4% of myocardial infarctions in young adults are triggered by • inborn abnormalities of coronary arteries • CASE PRESENTATION • ● 18 year old male presents from outlying facility with chest • pain and elevated Troponins • ● Obesity and tobacco use • ● EKG shows normal sinus rhythm with early repolarization • ● Patient diagnosed with NSTEMI as Troponin I trended down • from initial max of 10.3 ng/ml to 7.6 ng/ml upon arrival • Figure 1: Initial EKG on arrival from outside facility showing normal • sinus rhythm and early repolarization • Physical Examination showed: • ● Afebrile, 117/77, HR-70, R-16, O2 sat 100% • ● Obese male -BMI-38.6 kg/m2 • ● Lungs: CTA • ● Heart: RRR , no murmurs • ● Abdomen: Soft, non-tender, non-distended • ● Extremities: No pedal edema • ER Treatment: • ● Outlying facility gave Aspirin 81mg X4 and Toradol • ● Heparin drip was started with an initial bolus • ● CTA performed to rule out PE- negative • ● UDS/SDS negative • ● Repeat Troponin 5.9 ng/ml after 90 minutes • ● Chest X-ray – no cardiac enlargement or widen mediastinum Day 1: (admission) ● Stat Echo: Mildly enlarged right heart , EF 55%. Started on Heparin Drip. Placed in CCU. Day 2: ● Heart Catheterization: No occlusion, however anomalous right coronary Day 3: ● CTA of Coronaries: anomalous right coronary artery arising from left coronary cusp coursing between the aorta and pulmonary artery Figure 2: Left heart catheterization showing the origin of the RCA (yellow) arising from the left coronary cusp Day 4: ● Exercise NuclearStress test performed with stress images- negative for ischemia. Duke University consulted, patient transferred for surgical unroofing of anomalous right coronary artery Day 7: ● Patient had unroofing procedure and tolerated it well Day 10: ● Patient was discharged home DISCUSSION ● Anomalous right coronary artery is the second leading cause of sudden cardiac death in young athletes following hypertrophic cardiomyopathy ● Incidence is 0.17% ● Symptoms include chest pain, shortness of breath and diaphoresis ● Diagnosis is made through CTA of the coronary arteries or cardiac catheterization ● Treatment includes medical therapy/observation, stent deployment, or surgical correction Figure 3: CTA showing the RCA (yellow) courses between the aorta and pulmonary artery • 8 • CONCLUSION • ● Clinicians must be aware that young adults presenting with • sudden death, myocardial infarction, chest pain or syncope • may have coronary congenital anomalies. • ●Heightened awareness can lead to proper diagnosis and • treatment of an anomalous right coronary artery preventing • myocardial infarction or sudden death. References 1) Angelini, Paola MD. Congenital Heart Disease for the Adult Cardiologist; Coronary Artery Anomalies. Circulation 2007; 115:1296-1305. 2) Lee, Bae MD. Anomalous Right Coronary Artery from the Left Coronary Sinus: Is it Really Dangerous. Korean Circ J. May 2009; 39(5): 175-179. 3) National Center for Health Statistics.Health, United States, 2012: With Special Feature on Emergency Care Hyattsville, MD.2013 http://www.cdc.gov/nchs/data/hus/hus12.pdf#086 4) Premature Heart Disease. Harvard Men’s Health Watch. Nov 2009. http://www.health.harvard.edu/newsletters/Harvard_Mens_Health_Watch/2009/November/premature-heart-disease 5) Qin, Xuguang et al. Coronary Anomaly: Anomalous Right Coronary Originates from the Left Sinus of Valsalva and Coursing Between the Pulmonary Artery and Aorta. Clinical Interventions in Aging. 2013; 8:1217-1220. 6)Sudden Death in Young People: Heart Problems Often to Blame.Mayo Clinic. May 2011. http://www.mayoclinic.org/diseases-conditions/sudden-cardiac-arrest/in-depth/sudden-death/art-20047571?pg=2 7) Swaminath, Deephak et al. Anomalous Right Coronary Artery from Left Main Coronary Artery and Subsequent Coursing between the Aorta and Pulmonary Trunk. Case Reports in Medicine.2013; 2013: 195026.