Download
1 / 47
470 likes | 531 Views
Explore the reasons behind the need for change in vascular surgery training, focusing on technology interventions, training structure, professional performance, and public concern over surgical outcomes. Discover the gaps in training and how reforms can lead to improved care and lower mortality rates.

E N D
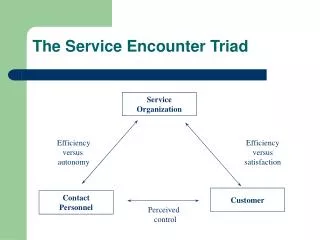
Service versus TrainingWho Wins? C P Shearman
Why Change? “I once found it quite stimulating but now it is just a job”
Interventions for leg ischaemia www.dh.gov.uk
2. Reason to change - Training So what is the problem! Who is going to do this? Formal Endovascular Training Complex open surgery Look if it was electric could I do this?
2. Reason to change - Training Unfinished Business 2002 • SHO training poorly structured • Inadequately supervised • No definitive end point • Needed Reform
Basic science+surgical skills Basic Imaging and IR skills Vascular biology Vascular medicine Professional skills Critical care Ultrasound Lower limb Venous Trauma Diabetes and vascular disease Aneurysms (aortic) Extra-cranial arterial disease Upper limb Visceral artery Renal vascular disease Vascular access Lymphodema Vascular malformations Congenital vascular disease Paediatric vascular Vascular Syllabus
Vascular Curriculum - Modular VASCULAR ACCESS Template 15
Reason to change – Professional Performance • Medical Expert/Clinical Decision Maker • Communicator • Collaborator • Manager • Health Advocate • Scholar • Professional The fuel light is on, Frank we are all going to die, we are all going to die. Whoops my mistake that’s the intercom light Medical Teacher 2000;22:549
European Working Time Directive 48 hours per week 1st August 2009 37 hours Denmark 80 hours United States
How Long to Train? Annual US trainee log book • Operating 2753 hours • Assisting 272 hours • Post op-care 938 hours total 3963 hours • 10-20,000 hours • Duration vs. competency • UK 2+6 years Purcell Jackson and Tarpley BMJ 2009;339:1069
Time to Train Modified from Purcell Jackson and Tarpley BMJ 2009;339:1069
Vascular Training in General Surgery? • Broad base • General Training • Skills acquired late • Shifts • Hospital at Night • Service Provision • Limited simulators
3. Case for Change - Outcomes The European Society for Vascular Surgery. (2008). Second Vascular Database Report
Volume / Outcome Relationship: Elective AAA Repair Holt et al, Br J Surg 2007
Variation in Amputation Rates Holt P et al BJS 2010 Holt P et al BJS 2010
Variation in Mortality Holt P et al BJS 2010 Holt P et al BJS 2010
Case for Change – Public Concern “Death rates in planned vascular surgery for abdominal aortic aneurysm (AAA – to prevent a burst artery) vary from under 2% in some hospitals to at least 10% in 10 of them.” “Patients are less likely to die in the bigger, busier hospital units where surgical teams are more skilled because they do more of the operations. The results strongly suggest that smaller units should close.”
Quality Improvement Framework for Aortic Aneurysms • MDT • radiology, anaesthetist, renal, cardiology • Procedures undertaken/supervised by consultant • 24/7 on site vascular cover • >33 cases per year • NVD • stop if >6% mortality
All hospitals and specialists comply with VSGBI QIF • Usually only one intervention centre with inpatient services • Screening Network for min 800,000 • Vascular specialists travel to intervention centre • Network provides full range of services for hospitals without vascular inpatients
5. Reason to change - Unmet need • Diabetes • Rising amputation rate cf. Finland • 68% no attempt at revascularisation before amputation • 3 million with diabetes 2010 • Carotid Surgery • 48hr access times • Under provision (15/100000) • Vascular Access • 17,140 per year • 66% by vascular teams • waiting list! • Cardiovascular Risk • 30% PAD patients risk factors treated
Trend in amputation in England and Wales 1996-2006 Type 2 Minor 95%↑ Major 83.5% ↑ Type 1 Minor 11.4%↓ Major 41% ↓ Vamos Diabetes Care and Clinical Research 2009
Amputation trends in People with Diabetes in Finland Incidence of 1st Amputation per 100,000 diabetics The number of 1st Amputations of diabetics in Finland 1988-2002 Lepantalo 2006
6. Reason to change - Emergency work • 30-40% of total workload • High risk • Cost • Immediate availability • Clinical Governance risk • Commissioners – SHA reviews • Specialty requirements • Endovascular rAAA • Out of hours imaging • Diabetic foot complications
Poor NHS care puts lives of emergency surgery patients 'at risk' • Report finds that delays in finding operating theatre spaces lead to deaths • while only one in three receives critical aftercare • Sam Jones and agencies • guardian.co.uk, Thursday 29 September 2011 09.02 BST • Article history
BBC News Hospital patients 'more likely to die at weekends' By Nick Triggle Health correspondent, BBC News A shortage of senior doctors is said to be at the heart of the problem Being admitted to hospital in England at the weekend is risky, experts say. A shortage of senior doctors is said to be at the heart of the problem
7. Reason to Change Manpower Anticipated number of trained specialists in General Surgery Headcount - HC NHS Workforce Review Team
8. Reason to change - Financial Expenditure • Highest spending since 1982–83 • Lowest tax burden since 1960–61 • Highest borrowing since WWII £178bn borrowing this year Receipts During the recession, government expenditure has continued to grow whilst receipts have fallen
What does this all mean? • Improve outcomes/quality • low volumes • AAA Screening • Adopt new technologies • endovascular • Training • More focused • Fewer trainees • Increased work load • diabetes • AAA screening • unmet need • Emergency provision • Clinical governance/consultant delivered • Financial downturn in NHS/save money Weasel didn’t like the sound of this
Solutions Hamster Health Care. Morrison I,Smith R. BMJ 2000 New ways of working “Interventions should be planned, executed and measured” • Training • Consultant role • Service structure Technology Redesign health care delivery
250 to learn to fly; 8 years to do an appendectomy Richard Reznick Accelerated pilot training: simulators
Solution 1 - Training • Simulators • Competency based • Relevant skills early • Service Focused • Disease focused Specific Skills Generic Skills
Solution 1 Training The Toronto Experiment 6 orthopaedic trainees • Early Entry into specialty training • Supernumerary to service • Early acquisition of skills • Progression by competency Richard Reznick
Make Training Cost Effective The other birds suspected Owl hadn’t worked in a DEANERY at all
Getting Value for Money • Professional Trainers • Job plan tariff + assessment • Standards for training units • Budget (£9.3m) • Withhold and invite bids • Competition for posts • Reward success eg ARCP1s
Fit for purpose training -Train for Service Core Training ST1-2 National Selection Intermediate Stage ST3-4 Vascular FRCS 1 Advanced Stage ST5-6 Vascular FRCS 2 Final Stage ST7-8 Standards for Vascular Training VSGBI 2011
Outline of the content of vascular specialty training Professional behaviour, leadership, teaching, audit, research Standards for Vascular Training 2011 VSGBI
Pre-specialty Training Role of Medical School, Foundation Schools service training?
NHS Employers Confederation • Role of Consultants • Front line delivery • Career structure/Teams • Systems Management • Quality improvement frameworks • IT and new technology • Utilisation of Facilities • 6-7 day working • Step down beds • Outcome based standards • mortality • Commissioning Standards • national • providers met www.nhsconfed.org/publications
Consultant Working Practice – value for money • No elective commitments • Daily unit ward round • Emergency walk in clinic • Emergency list • Evening ward round Reduce admissions Reduce length of stay Allow better training Value for money Intermediate/complex consultants Added value Routine trainees
Solution 3 - Restructuring of Services High quality, cost effective, sustainable • Fewer, larger units (50) • Consultant teams - min 6 (8-9) • Change in consultant role • Service delivery • Sub-specialisation (EVAR vs Open) • Designated trainers • Surgeon specific outcomes (NVD) • Fewer Trainees (1per unit?) Provision of Services for Patients with Vascular Disease VSGBI 2011
Solution – Centralisation “There is evidence that even with transfers of more than one hour, transfer to a vascular unit improves patient outcomes” “Centralisation…is the preferred method of providing high standard vascular services” “There has been little strategic planning in the way vascular services are commissioned and delivered. As far back as the original Provision of Vascular Services document, it was recommended that coalescence of adjacent vascular services onto a single site is the optimal model for service delivery” “Access to specialist care will often involve transfer of patients to the nearest hospital where emergency vascular treatment is available. In certain geographical areas this may involve travelling some distance, but there is good evidence that patient outcomes are not related to the distance travelled if they reach a centre where vascular expertise is available”
A Bright Future • Embrace service change • Role of consultant • Focus on training needs • Training fit for service “What do you mean it’s a bit muddy!”