Download
1 / 41
530 likes | 1.26k Views
Treatment Options for Phantom Limb Pain. By: Sara Walsh, SPT Ithaca College. Objectives. Background information on phantom pain Mirror Therapy Virtual Reality Therapy Current Evidence Speculations. What exactly is phantom limb pain?.

E N D
Treatment Options for Phantom Limb Pain By: Sara Walsh, SPT Ithaca College
Objectives • Background information on phantom pain • Mirror Therapy • Virtual Reality Therapy • Current Evidence • Speculations
What exactly is phantom limb pain? • Any painful sensation perceived in the missing part of the limb after amputation • Not to be confused with phantom sensation or residual limb pain • Stabbing, cramping, burning 1
Why do we care about phantom limb pain? • Chronic phantom limb pain is present in 80% of individuals with partial or total limb loss. • 156,000 new amputations per year • 156,000 x 0.80 = 124,800 1,2
Why does phantom pain occur? • Historically: psychological origins • Overall abnormal overload of input to the spinal cord and brain 1 3,1
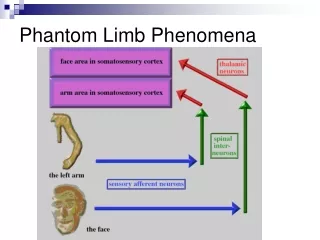
Why does phantom pain occur? • Peripheral Mechanism • Many theories • Pain from neuroma increases the amount of central map reorganization; reorganization=pain • Enhanced sensitivity of afferent fibers (toward CNS) • Local changes at site of remaining nerve • Enhanced sensitivity • Sprouting of injured axon: neuroma • Spinal cord forming new neural connections with sprouts (contributes to sensitization of pain transmission neurons) • Reduction of local inter-segmental inhibitory mechanisms: spinal dis-inhibition and enhanced supra-spinal input to nociceptive centers 1
Why does phantom limb pain occur? • Central Mechanism • Changes in neuronal excitability (motor activation without sensory feedback to dampen motor commands verifying that movement has taken place • Somatotopic reorganization in cortical and subcortical areas • Neuroimaging studies reveal that a reversal of these neuroplastic changes are associated with phantom limb pain remission 1, 3 3
Pharmacological Treatment • NSAIDS • Most evidence based • Anti-depressants • Anticonvulsants • Sodium Channel blockers • NMDA receptor antagonists (anesthesia) • Opioids 4
Invasive Treatments • Must consider possible side effects of neurosurgery (wound infection, device failure, wire migration, anesthesia, stroke, death) • Invasive Neuromodulation (last resort) • Deep brain stimulation (stimulate thalamus) • <25% success rate • Motor Cortex stimulation • Precentralgyrus • 53% success rate • Spinal Cord Stimulation • Electrodes in epidural space • 39% success rate 5,6,7
Non-Invasive Treatments(low levels of evidence) • Trans-cranial magnetic stimulation (TMS) • Electrical currents due to magnetic coil over scalp • Electrical Stimulation • Psychotherapeutic approaches • Reflexology • Hypnosis • Motor Imagery (moderate levels of evidence) • Myoelectric Prosthesis • Expansion of representation zone 4
Mirror TherapyHow does it work? • Mirror Neuron System • Neurons are active during execution of tasks and during observation of tasks • Imagined movements share the same cortical pathways as executed motor tasks • Visual feedback dominates somatosensory feedback • Sensory experiences can be evoked by visual information • Visual system enhances tactile sensitivity 8,9
Mirror Therapy • Current Evidence: • 3 case reports on pts. with UE amputations • Kawashima 2009 • Wilcher 2011 • 2 case studies on p.t with LE amputation • MacLauchlan 2004 • Darnall 2009 • Darnall 2012 • 2 RCTs on pts. with LE amputations • Chan 2007 • Brodie 2003 • 1 quasi-experimental study on pt. with LE amputation • Seidel 2011 10-16
Mirror Therapy • Subjects: • Males and females • 24-83 y/o • Mechanism of Injury • Trauma • UE caught in machine at work • Motorcycle accident • Necrotizing Fasciitis • DM • Vascular disease 10-16
Mirror Therapy • Typical Protocol • Pt. is seated with mirror oriented to pt.’s sagittal plane so that pt. can see sound limb’s reflection in mirror (resembles phantom limb) • Synchronous movements • Elbow, Wrist flex/extension • Opening/closing fist • Pronating/supinating • Clapping (with someone else making “clapping noise”) • Hip, Knee flex/extension • DF/PF, inversion/eversion, circumduction ankle • Seated marches • Flex/extension toes • Spread toes/relax toes, Ext great toe while flexing other toes • Hip abduction/adduction, Hip ER/IR • 15 minutes 2x/day to 1 hour/week • 1 month - 3 months 10-16
Mirror Therapy • Results: • Metal bar grasped by phantom limb with severe pain …did not feel existence of phantom (Kawashima-case study UE amp) …EMG modulations in residual wrist mm. (pt able to re-activate commands to phantom limb • Naproxin, tramadol, morphine, acetaminophen, lidocaine, gabapentin…all pain meds except gabapentin discontinued and blood pressure decreased (as a sign of decreased pain) (Wilcher-case study UE amp) • 5-9/10 pain…0-1/10 with 0 % control over phantom limb to 25-30% control over phantom limb (MacLaughlen-case study LE amp) • After 4 wks, 100% of pts in mirror group had decreased pain and phantom limb pain decreased in 8/9 pts who switched to mirror therapy from covered mirror of mental visualization (Chan-UE and LE RCT) • 3 fold increase in amount of movement perceived vs. control group, but no decrease in pain b/c all but one pt was not in pain at the time of the study (Brodie-UE and LE amps RCT) • 6/10 – 0/10 pain with increased control of phantom (Darnall-case study LE amp) • 15 % pain reduction in 2 months (Darnall-Case study LE amp) • 4.6/10 pain…1.8/10 pain (statistically significant) • No consistent pattern of cortical reorganization (Seidel-quasi LE) 10-16
Trivia Question for Candy #1 • Mirror therapy has been proven to be effective in: • A) the clinic • B) the home setting • C) both the clinic and the home setting
Answer: • C) both the clinic and the home setting
Mirror TherapyConclusions • Mirror therapy is a non-expensive (third party payer,) noninvasive option for phantom limb pain management • Statistically significant reductions in pain • Mirror therapy can be used on UE and LE amputees • Increased control of phantom = decrease in pain • Use with patients who are currently having pain • Home PT • ***More high quality evidence is needed*** 10-15
Virtual Reality Therapy • Limited quantity of evidence (2 studies) • Case Study/Quasi-experimental Murray • Quasi-experimental (1 group pretest post-test) • Subjects ->pre-test measurement->intervention -> post test measurement-Cole • Qualitative component • Unable to rate on hierarch, but resembles a 2b for quasi-experimental (on a scale of 1a-5) • 3B-case study • Lacks randomization and control group 17,18
Virtual Reality Therapy • Based on principles of mirror therapy • Addresses limitation of mirror therapy • Narrow spatial dimension • Patient in fixed space • Patient must ignore intact limb providing the reflection 17,18
Virtual Reality Therapy • Murray-2007 and Cole-2009 • Quasi-experimental studies • Murray: 3 pts in their 60’s (2 UE amps and 1 LE amp) • Cole: 14 pts ages 27-82 (7 UE amps and 7 LE amps) • Inclusion Criteria (Murray): • Has phantom limb pain • Adults without any major visual or cognitive deficits • Minimum 12 months post–amp 17, 18
Virtual Reality Therapy • Murray Protocol: • 2-5 immersive virtual reality sessions (30 mins each) • V6 virtual reality head-mounted display, 5DT-14 data glove and sensors with UE amp and just sensors for LE amps (sensors attached to elbow, wrist, knee, ankle) • four tasks in repetition • placing virtual limb onto colored tiles which light up in sequence • batting or kicking a virtual ball • tracking the motion of a moving virtual stimulus • directing a virtual stimulus toward a target 17
Virtual Reality Therapy • Cole Protocol: • UE: seen twice, several weeks apart • LE: seen once • 60-90 mins • Motion capture device respond to electro magnetic sensors attached to arm/leg of user • Calibrate system through set of residual limb movements • Grasp apple on surface of a table • Bass drum: LE 18
Virtual Reality Therapy • Outcome measures: • Short form McGill Pain Questionnaire (Murray and Cole) • VAS pain scale (Murray and Cole) • Pain diaries (Murray) • Drug use (Cole) • Qualitative component: semi-structured interview before and after each session (Murray and Cole) 17,18
Virtual Reality Therapy • Results • 8.3/10 -> 6.8/10 Murray • 5-6 hrs of sleep compared to 2-3 Murray • 7/10 to 3/10 at third session Murray 17, 18
Virtual Reality Therapy • Testimonials: UE • Reported decrease in pain, but then it would come back with “a bit of a vengeance” within a few hours • “I actually felt as if it was my left arm that was doing the work and chasing the ball. My actual phantom arm rather than my right…and was more like reality than virtual reality.” • “If I could harness that movement in my phantom limb maybe I could open my fingers and ease the cramping pain a little.” • “I’ve actually been sleeping a little better over the last few days…I’m getting about 5-6 hours of sleep as opposed to 2-3 hours and I’m doing nothing else different in my life except coming here • “It’s funny, one of my fingers is coming out, sort of pointing out now versus: the nails of my fingers are digging into my palm” • “Now when I move the fingers there is still pressure but there is no pain, they are not being ripped off or squashed.” • “When I move my arm, it does not tingle; pain disappears into the background and merges into the movement sensations • “The arm is now a gentle presence.” 17, 18
Virtual Reality Therapy • Testimonials: LE • “I can feel the movement in the missing leg and maybe feel touch too. Once I am on the pedal I relax and feel my foot coming off it. It is second nature as though moving my full leg. The prosthesis is always a prosthesis; this is different. Here I am moving the foot. And at the moment the toes have sensation and though there is slight cramping in the toes there is no pain.” (pain went from 7-0) • “It is no longer a constant throbbing. When I stop moving the pain returns within a second or two , but equally when I move and feel it is me, the pain reduces. (LE) 17, 18
Virtual Reality Therapy 17, 18 • Should we consider using this evidence with our pts?
Trivia Question for candy # 2 • Name 2 evidence based outcome measures you could use if you were treating a patient with virtual reality therapy……
Possible Answers: • Short form McGill Pain questionnaire • VAS scale • Pain diaries • Medication dosages
Virtual Reality Therapy • Conclusions: • Expensive (third party payer) • Decrease in pain • Lack of carryover • Patient satisfaction • Need for increased research • Promising starting point • Look for future research 17, 18
Trivia Question #3 for candy: • There is a specific protocol to follow for mirror therapy and virtual reality therapy • True or False
Answer: • False
Speculations • Virtual reality/mirror therapy with prosthetic training • Virtual Reality Therapy vs. Mirror Therapy vs. Control Group • Large Sample Sizes • High Quality RCT
Thank You! • Any questions? • Please fill out my survey
Works Cited • FlorH. Phantom-limp pain: characteristics, causes and treatments. Lancet Neurol. 2002;1(3):182-189 • American Amputee Foundation, Inc. AAF. http://www.americanamputee.org/. Accessed August 26, 2012 • Maclver K, Lloyd M, Kelly S, Nurmikko T. Phantom limb pain, cortical reorganization and the therapeutic effect of mental imagery. Brain. 2008;131:2181-2191. • Knotkova H, Cruciani R, Tronnier V, Rasche D. Current and future options for the management of phantom-limb pain. Journal Of Pain Research 2012;5:39-49. Available from: MEDLINE, Ipswich, MA. Accessed July 22, 2012 • Rasche D, Ruppolt M, Stippich C, Unterberg A, Tronnier VM. Motor cortex stimulation for long-term relief of chronic neuropathic pain: a 10 year experience. Pain 2006;121(2):43-52 • Nguyen JP, Nizard J, Keravel Y, Lefaucheur JP. Invasive brain stimulation for the treatment of neuropathic pain. Nat Rev Neurol. 2011;7(12):699-709 • Krainick JU, Thoder U. Spinal cord stimulation in post-amputation pain. In: Siegfried J, Zimmerman M, editors. Phantom and Stump Pain. Berlin, Germany: Springer-Verlag; 2002:527-535 • Cole J, Crowle S, Austwick G, Slater D. Exploratory findings with virtual reality for phantom limb pain; from stump motion to agency and analgesia. Disability And Rehabilitation[serial online]. 2009;31(10):846-854. Available from: MEDLINE, Ipswich, MA. Accessed August 26, 2012 • Diers M, Christmann C, Koeppe C, Ruf M, Flor H. Morrored, imagined and executed movements differentially activate sensorimotor cortex in amputees with and without phantom limb pain. Pain. 2010;149(2):296-304 • Kawashima N, Mita T. Metal bar prevents phantom limb motion: case study of an amputation patient who showed a profound change in the awareness of his phantom limb.Neurocase [serial online]. December 2009;15(6):478-484. Available from: MEDLINE, Ipswich, MA. Accessed August 26, 201 • Wilcher D, Chernev I, Yan K. Combined mirror visual and auditory feedback therapy for upper limb phantom pain: a case report. Journal Of Medical Case Reports [serial online]. January 27, 2011;5:41. Available from: MEDLINE, Ipswich, MA. Accessed August 26, 2012
Works Cited • MacLachlan M, McDonald D, Waloch J. Mirror treatment of lower limb phantom pain: a case study. Disability And Rehabilitation [serial online]. 2004 Jul 22-Aug 5 2004;26(14-15):901-904. Available from: MEDLINE, Ipswich, MA. Accessed August 26, 201 • Chan B, Witt R, Tsao J, et al. Mirror therapy for phantom limb pain. The New England Journal Of Medicine [serial online]. November 22, 2007;357(21):2206-2207. Available from: MEDLINE, Ipswich, MA. Accessed August 26, 2012 • Brodie E, Whyte A, Waller B. Increased motor control of a phantom leg in humans results from the visual feedback of a virtual leg. Neuroscience Letters [serial online]. May 1, 2003;341(2):167-169. Available from: MEDLINE, Ipswich, MA. Accessed August 26, 2012 • Seidel S, Kasprian G, Prayer D, et al. Mirror therapy in lower limb amputees--a look beyond primary motor cortex reorganization. Röfo: Fortschritte Auf Dem Gebiete Der Röntgenstrahlen Und Der Nuklearmedizin [serial online]. November 2011;183(11):1051-1057. Available from: MEDLINE, Ipswich, MA. Accessed July 22, 2012 • Darnall, BD. Self-delivered home-based mirror therapy for lower limb phantom pain. American Journal of Physical Medicine and Rehabilitation. 2009;88:78-81. • Darnall, B, Li H. Home based self delivered mirror therapy for phantom pain: a pilot study. J Rehabil Med. 2012; 44: 254-260 • Murray C, Pettifer S, Bamford C, et al. The treatment of phantom limb pain using immersive virtual reality: three case studies. Disability And Rehabilitation [serial online]. September 30, 2007;29(18):1465-1469. Available from: MEDLINE, Ipswich, MA. Accessed August 26, 2012 • Cole J, Crowle S, Austwick G, Slater D. Exploratory findings with virtual reality for phantom limb pain; from stump motion to agency and analgesia. Disability And Rehabilitation[serial online]. 2009;31(10):846-854. Available from: MEDLINE, Ipswich, MA. Accessed August 26, 2012