Download
1 / 2
20 likes | 220 Views
II. attach PID label here. -. -. Patient ID:. Clinical Unit:. -. -. Month. Day. Year. 2. 2. 2. 1. 1. 1. 2. 1. 1. 2. 2. 2. 1. 1. Yes. No. No. pounds. kilograms. Yes. Yes. Yes. Yes. No. No. inches. centimeters. No. Form Date:. Coordinator Code:. Visit:.

E N D
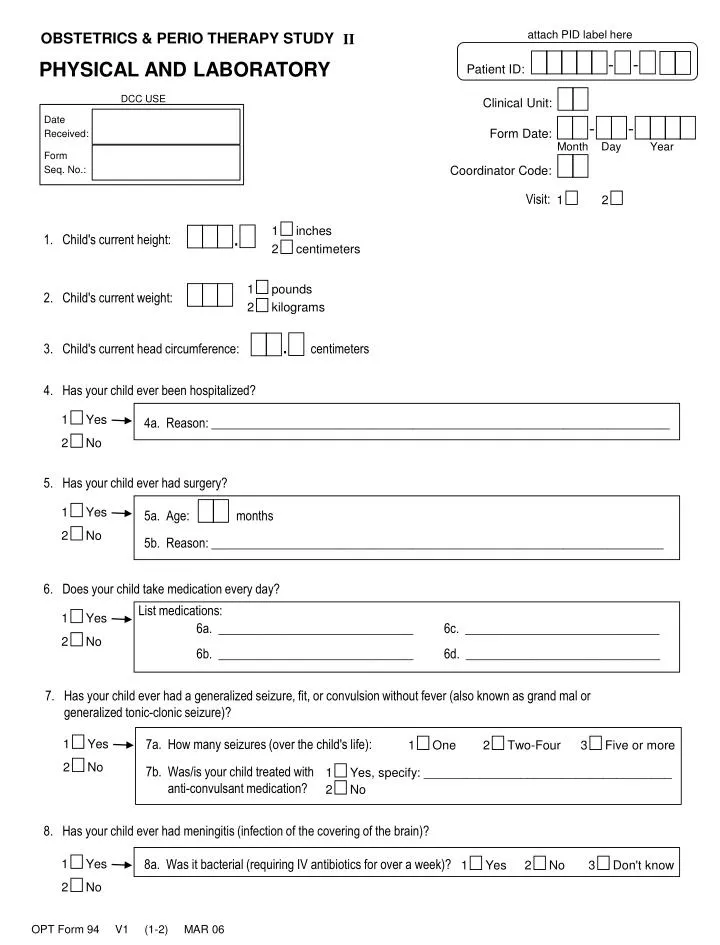
II attach PID label here - - Patient ID: Clinical Unit: - - Month Day Year 2 2 2 1 1 1 2 1 1 2 2 2 1 1 Yes No No pounds kilograms Yes Yes Yes Yes No No inches centimeters No Form Date: Coordinator Code: Visit: 2. Child's current weight: . 1. Child's current height: 1 2 . 3. Child's current head circumference: centimeters 4. Has your child ever been hospitalized? 4a. Reason: _________________________________________________________________________ 5. Has your child ever had surgery? 5a. Age: months 5b. Reason: ________________________________________________________________________ 6. Does your child take medication every day? List medications: 6c. _______________________________ 6a. _______________________________ 6b. _______________________________ 6d. _______________________________ 7. Has your child ever had a generalized seizure, fit, or convulsion without fever (also known as grand mal or generalized tonic-clonic seizure)? 7a. How many seizures (over the child's life): 7b. Was/is your child treated with anti-convulsant medication? 8. Has your child ever had meningitis (infection of the covering of the brain)? 8a. Was it bacterial (requiring IV antibiotics for over a week)? 3 1 2 1 3 2 1 2 Five or more Yes No One Two-Four No Yes, specify: ____________________________________ Don't know PHYSICAL AND LABORATORY OPT Form 94 V1 (1-2) MAR 06
II - - Patient ID: 9. Has your child ever had encephalitis (a viral infection of the brain often accompanied by seizures)? 1 2 2 1 1 2 2 1 1 1 2 2 2 1 1 2 Yes No No Yes No Yes No Yes No No Yes Yes No Yes Yes No 10. Has your child ever had ear infections? 10a. How many infections has your child had over the last six months? 10b. Did your child have tubes placed in his/her ear? 11. Has your child ever had a head injury? 11a. Did your child lose consciousness? 11b. Did your child have a skull fracture? 12. Is this Visit One? STOP. DO NOT DRAW BLOOD. 13. Was venous blood drawn? 13a. Was sufficient blood drawn for all analyses? 13b. Reason: _______________________________________________________________________ Lab did not provide this value µg/dL % 103/µL g/dL 106/µL fL pg g/dL 1 1 1 1 1 1 1 1 1 1 1 % 103/µL fL 1 2 No Yes 14. Blood results: a. Lead level: b. Hematocrit (Hct): c. White blood count (WBC): d. Hemoglobin (Hb): e. Red blood count (RBC): f. Mean cell volume (MCV): g. Mean cell hemoglobin (MCH): h. Mean cell hemoglobin concentration (McHc): i. Relative or red cell distribution width (RDW): j. Platelets (PLT) k. Mean platelet volume (MPV): OPT Form 94 V1 (2-2) MAR 06