Download
1 / 20
200 likes | 296 Views
Rapid and Slow Fibrosers in Chronic HCV Infection. Dr Saeed Hamid Professor & Chair Department Of Medicine The Aga Khan University Karachi, Pakistan. Natural History of Fibrosis progression in chronic HCV.

E N D
Rapid and Slow Fibrosers in Chronic HCV Infection DrSaeed Hamid Professor & Chair Department Of Medicine The Aga Khan University Karachi, Pakistan
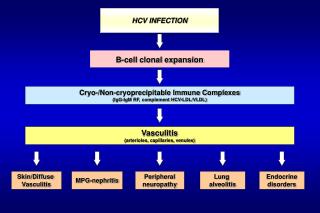
Natural History of Fibrosis progression in chronic HCV • The natural history of patients with chronic hepatitis C is characterized by a slow progression of liver fibrosis. • Cirrhosis may develop after an average of 20 to 30 years. • In some patients, the rate of fibrosis progression is much faster and cirrhosis develops after 10 to 15 years. • The pathogenesis of HCV-induced liver fibrosis is now better understood. • HCV infects hepatocytes, causing oxidative stress and inducing the recruitment of inflammatory cells, which leads to HSC activation and collagen deposition. • The HCV core protein stimulates secretion of pro-fibrogeniccytokines by hepatocytes. Rockey, SeminGastrointestDis 2000; Bataller, Hepatology2002; 2003
Challenges in the study of fibrosis progression in CHC • Time of infection is often not clear. • Not many prospective studies available. • Assumptions that fibrosis progression is linear
Rate of Progression of Hepatic Fibrosis: The HALT-C Study • “fast” progression:1 Ishakstage ≤5 years • “slow” progression: 1 stage in ≥ 5 years. Hoefs, Gastro 2011
Clinical correlates between rapid and slow progressors • Rapid progressorshad more advanced CLD at baseline (P≤.0001) • More frequent evidence of hepaticinjury (↑AST, ALT, AFP), with no correlation to histologic inflammation. • Fast progressorswere almost 5 times more likely to experience a clinical outcome. Hoefs, Gastro 2011
Liver fibrosis progression in patients with chronic HCV • rapid ‘‘fibrosers’’ (median • time to cirrhosis <20 yrs) • slow ‘‘fibrosers’’ (median time to cirrhosis >50 yrs Poynard, Lancet 1997
Linear regression model to analysepredictors for rate of fibrosis Wright, et al, Gut 2003
Regulation of gene expression in hepatic stellate cells during fibrosis Hernandez-Gea, Annu. Rev. Pathol. Mech. Dis. 2011
Pathogenesis of liver fibrosis and sites of action of studied candidate genes Bataller, Hepatology 2003
Main Cytokine pathways regulating liver fibrosis Hernandez-Gea, Annu. Rev. Pathol. Mech. Dis. 2011
Gene Polymorphisms That Influence Progression of Liver Fibrosis in Humans Bataller, Hepatology 2003
Fibrosis Progression rate (units/year) related to TGFb1 genotypes of the four polymorphisms • 48 patients of whom the exact time point • of HCV-infection could be assessed • Progression calculated as the ratio between fibrosis stageat time of biopsy and the • estimated duration of infection The heterozygous ArgProof codon 25 predicts significantly faster fibrotic progression than the homozygous 25ArgArg genotype Location of presently known polymorphisms in the TGF-b1 gene Gewaltig , ClinicaChimicaActa2002
Distributionof IL-10 genotypes among fast vs slow fibrosis progressors • Fibrosis rate= fibrosis score/years of infection • Male gender and age at infection (<40) were associated with rapid fibrosis IL-10 (1082) AA genotype (low IL-10 producing genotype) and the ATA/ATA and ACC/ACC homozygous haplotypes were more frequent among patients with rapid fibrosis. Knapp, Immunogenetics (2003)
Progression According to Initial Fibrosis Stage and Cirrhosis Risk Score • 271 untreated patients with chronic hepatitis C, METAVIR stage F0 (n=104), • F1 (n=101), or F2 (n=59), followed up for at least 5 years. • 7 SNPs contributed to the CRS, (low risk, CRS 0.5; moderate risk, CRS 0.5-0.7; high risk, CRS 0.7). The association of CRS score with fibrosis progression was highly significant in male patients Marcolongo, Hepatology2009
Mannose-Binding Lectin Polymorphisms in Patients with HCV Infection • Variations in mannose-binding lectin and specific HLA-II alleles (DRB1*0405-DQB1*0401), which are involved in host defense against viral infections, also influence cirrhosis development. Sasaki,Scand J Gastroenterol 2000
TAP2*0201 Allele and risk of early cirrhosis • Transporter Associated With Antigen Processing 2 plays an important role in the antigen processing system where it translocates antigenic peptides from the cytosol into the endoplasmic reticulum. Akuta, J Med Virol 2001
Fast Fibrosis Progression in HIV/HCV Co-infected patients • Over a 3 year period, 44%of patients progressed one or more stages of fibrosis. • Progression of fibrosis was predicted by - the degree of necrosis and inflammation in the first biopsy. - ETR with anti-HCV therapy and - suppression of HIV replication • gp120 or inactivated HIV enhanced TGF-beta 1 expression in both uninfected and HCV-infected hepatocytes Macı´as, HEPATOLOGY 2009
Conclusions • Major advances in characterizing the geneticdeterminants of fibrosis progression. • To use them clinically as effective prognostic parameters has been a challenge. Some potential uses would be: - Tailor follow up - Timing of specific therapy - Design of clinical trials Friedman, Nature Reviews 2010
Consensus Recommendation • Clinical and Demographic factors for fibrosis progression are well defined and have worked well over time (A) • Although many genetic markers are now defined for prediction of fibrosis progression, more prospective randomized data is required before these markers can be recommended for general clinical use. (B, 2) • Genetic markers can be very helpful in the conduct of therapeutic trials of fibrosis therapy, and should be routinely included in clinical trials of anti-fibrotic therapy (B, 1).