Download
1 / 59
610 likes | 827 Views
The person who asks a foolish question is a fool for 5 minutes, the one who doesn't ask a question remains a fool forever. Why liquefactive necrosis in Brain ?. Because brain cells are rich in lipids and digestive hydrolytic enzymes, the brain cells are digested by their own hydrolases

E N D
The person who asks a foolish question is a fool for 5 minutes, the one who doesn't ask a question remains a fool forever....
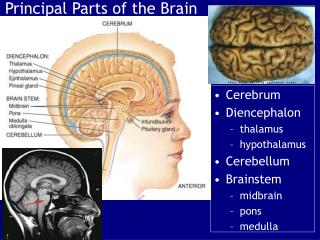
Why liquefactive necrosis in Brain ? • Because brain cells are rich in lipids and digestive hydrolytic enzymes, the brain cells are digested by their own hydrolases • The brain tissue becomes soft, liquefies, and is walled off from the healthy tissue to form cysts
Liquefactive necrosis can also result from bacterial infections. • Here, the hydrolases are released from the lysosomes of phagocytic neutrophils that are attracted to the infected area to kill the bacteria;
Definition Detached, intravascular, solid, liquid or gaseous mass that is carried by the blood to a site distant from its point of origin
Usually dislodged THROMBUS (platelets + fibrin + RBC’s + degenerating WBC’s)
Droplets of fat • Bubbles of air / nitrogen • Cholesterol (atherosclerotic debris) • Tumour fragments • Bits of bone marrow • Foreign bodies
An embolism is usually thrombotic unless otherwise specifiedThromboembolism
TYPES • Pulmonary embolism • 2. Systemic embolism • Amniotic fluid embolism • Air embolism • Fat embolism
PULMONARY THROMBOEMBOLISM • Majority – clinically silent (60-80%), undergo organization • If > 60% of pulmonary circulation is obstructed => SUDDEN DEATH, RHF
PULMONARY EMBOLISM • More than 95% - the venous emboli arise from the deep leg vein thrombi above the level of the knee • Main pulmonary trunk • Saddle emboli • Smaller branches • Small multiple emboli
PULMONARY THROMBOEMBOLISM • If medium sized vessels : usually haemorrhage, no infarction • If small end arteriole : infarction • Multiple emboli : PHT with RHF
Causes • cardiac diseases • cancer • prolonged immobilization • Hypercoagulable states
Clinical significance depends on • Extent of emboli • Number of emboli • Circulatory state
FATE OF EMBOLI • may resolve by fibrinolysis • unresolved • pulmonary H T • pulmonary vascular sclerosis • chronic cor pulmonale • 30 % chance of developing second emboli
Prophylaxis: • Elevation • Elastic bandage • Early ambulation • Embolectomy • UMBRELLA filter in inferior vena cava • Thrombolysis followed by anti coagulation with monitoring
SYSTEMIC EMBOLISM Embolism in arterial circulation. • SOURCE : 80 – 85 % from heart • 60 -65 % from left ventricle ( intracardiac mural thrombi) • 5 – 10 % rheumatic heart disease • 5% cardiomyopathy
SYSTEMIC EMBOLISM • OTHER LESS COMMON SOURCES • Atherosclerotic plaques • Aortic aneurysms • Infective endocarditis • Valvular heart diseases • Paradoxical emboli from venous thrombi • UNKNOWN SOURCES 10 – 15 %
PARADOXICAL EMBOLISM
Always cause infarction • SITES : • Lower extremities 70 -75 % (gangrene) • Brain 10 % • Viscera 10 % • Upper limb 7 – 8 %
Factors • collateral vascular supply • tissue’s vulnerability to ischaemia • caliber of occluded vessel
Clinical manifestations : site and size of emboli is important femoral artery - gangrene cerebral artery (MCA) - death in hrs/ days • Treatment : anticoagulants embolectomy
AMNIOTIC FLUID EMBOLISM • Rare complication of labor • Major cause of maternal mortality • 86% mortality
AMNIOTIC FLUID EMBOLISM • Cause : Tear in placental membrane or rupture of uterine / cervical veins leading to infusion of amniotic fluid or fetal tissue into the maternal circulation
CLINICAL FEATURES: • Deep cyanosis • C.V.S shock • Generalized convulsions • Coma • Excessive bleeding from birth canal • DIC (due to release of thromboplastic substances)
AMNIOTIC FLUID EMBOLISM • The pulmonary microcirculation may contain: -squamous epithelium of fetal skin -fat from vernix caseosa -mucin from fetal respiratory and GIT -bile from meconium stained amniotic fluid
AMNIOTIC FLUID EMBOLISM • Investigations : • X-ray evidence in 24 – 36 hours • Pul. perfusion lung scan alb-labeled with Tec99 • Investigation of choice : pulmonary angiography
AIR OR GAS EMBOLISM • Bubbles of air or gas obstructing circulation • During obstetric procedures • Chest wall injury • >100 cc to produce clinical effect • Tissue damage
2 types • Acute • Chronic - decompression disease Acute • “Bends” - obstruction of small vessels around joints and skeletal muscles cause patients to double up with pain • “Chokes” - respiratory and brain involvement sudden death
Caisson disease or decompression sickness- at risk : scuba divers, workers in offshore drilling platforms, underwater tunneling system workers
When air embolism is suspected at autopsy organs should be opened under water to detect escaping gas.
FAT EMBOLISM • Fat Emboli were first noted by F.A. Zenker in 1861 in a railroad worker with a thoraco-lumbar crush injury • The Fat Embolism Syndrome (FES) was first described by Von Bergman in 1873 in a diagnosis confirmed by post mortem examination. This patient had a fractured femur