Download
1 / 10

E N D
kidney cancer treatment Byhttp://kidneycancersurvivalrate.net/kidney-cancer-treatment
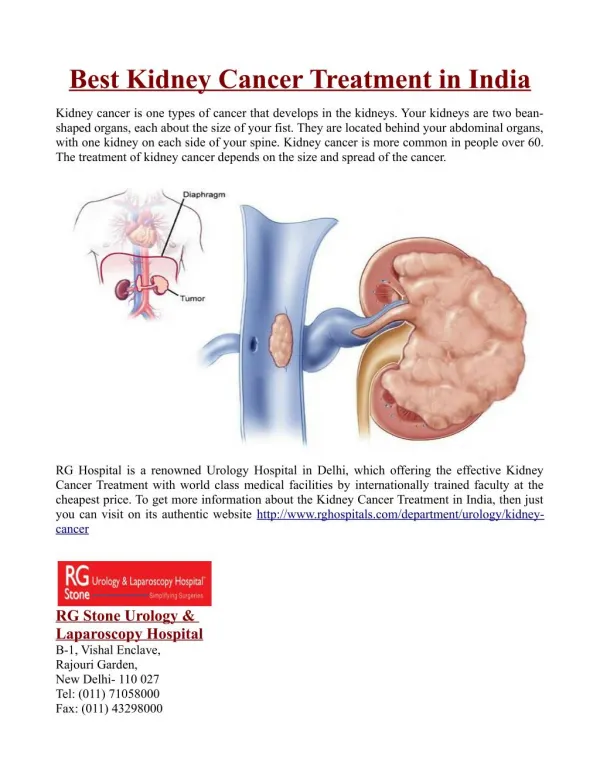
The treatment options of renal cell carcinoma vary from patient to patient - two patients are exactly alike, treatment and responses to treatment vary greatly. It depends on many factors, such as the tumor size and location, type of the RCC (Clear Cell RCC, Papillary RCC, etc.), the general health state of the patient. One of the most important factors is the cancer stage. First of all, click to check this simplified stage form and you need to be sure about the cancer stage before continuing.
Stage I and stage II: • Patients with stage I and II RCC often have their cancers surgically removed by either removes parts of the kidney or the entire kidney is called nephrectomy. Other than as part of a clinical trial, additional (adjuvant) treatments such as targeted therapy, chemotherapy, radiation therapy, or immunotherapy after surgery for stage I or stage II RCC are usually not recommended, as the benefit of additional therapy has not been proven.
Patients who are unable to have surgery because of other serious medical problems are often treated by other local treatment such as cryoablation, radiofrequency ablation, or arterial embolization. With surgical treatment, the 5-year survival for stage I patients is between 88% and 100% and 65% to 75% for stage II.
Stage III: • Radical nephrectomy is the most common treatment option for stage III RCC. Sometimes, a patient will have an arterial embolization procedure in attempt to reduce the amount of bleeding during nephrectomy. There is no distant metastasis in stage III, however if the cancer extends into nearby veins, the surgeon may need to cut open these veins and to completely remove the cancer. The 5-year survival for stage III patients varies widely and is between 40% and 70%, depending on the local extent of the cancer.
Stage IV:, IL-2, and everolimus. • Treatment of stage IV kidney cancer depends on how extensive the cancer is and on the person's general health. In some cases, surgery may still be a choice. When one or a few metastases are present and the surgeon considers it possible to remove them without serious side effects, an aggressive surgical approach to removing the kidney tumor and these metastases may be beneficial. For cancers that can't be removed surgically (because of the extent of the tumor or a person's health), first-line treatment would likely be one of the targeted therapies or cytokine therapy.
For some patients, palliative treatments such as embolization or radiation therapy may be the best option. Surgery or radiation therapy can also be used to help reduce pain or other symptoms of metastases in some other places, such as the bones. (How to relieve cancer pain)
Recurrent RCC • In rare cases, a patient will have a solitary site of recurrence of RCC detected several years after nephrectomy. In these exceptional cases, surgical removal of the solitary site of recurrence may be possible after extensive imaging tests have shown no other evidence of cancer spread. Otherwise, treatment with targeted therapies or cytokine immunotherapy will be recommended. Clinical trials of new treatments are an option as well.
Beat Renal Cell Carcinoma [http://www.beatrcc.com/] is a great website which provides all kinds of information about kidney cancer (Renal Cell Carcinoma), including causes, symptoms, diagnosis, staging, diet & nutrition, treatment and prognosis, and other related topics such as qigong, traditional Chinese medicine, etc.
kidney cancer treatment For more information, please visit http://kidneycancersurvivalrate.net/kidney-cancer-treatment