Download
1 / 1
10 likes | 122 Views
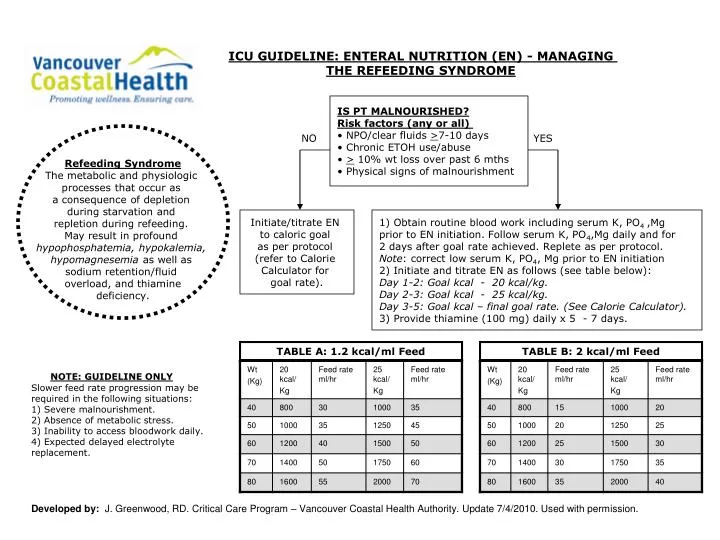
ICU GUIDELINE: ENTERAL NUTRITION (EN) - MANAGING THE REFEEDING SYNDROME. IS PT MALNOURISHED? Risk factors (any or all) NPO/clear fluids > 7-10 days Chronic ETOH use/abuse > 10% wt loss over past 6 mths Physical signs of malnourishment.

E N D
ICU GUIDELINE: ENTERAL NUTRITION (EN) - MANAGING THE REFEEDING SYNDROME IS PT MALNOURISHED?Risk factors (any or all) • NPO/clear fluids >7-10 days • Chronic ETOH use/abuse • > 10% wt loss over past 6 mths • Physical signs of malnourishment Refeeding SyndromeThe metabolic and physiologic processes that occur as a consequence of depletion during starvation and repletion during refeeding. May result in profound hypophosphatemia, hypokalemia, hypomagnesemia as well as sodium retention/fluid overload, and thiaminedeficiency. NO YES Initiate/titrate EN to caloric goal as per protocol (refer to Calorie Calculator for goal rate). 1) Obtain routine blood work including serum K, PO4 ,Mg prior to EN initiation. Follow serum K, PO4,Mg daily and for 2 days after goal rate achieved. Replete as per protocol. Note: correct low serum K, PO4, Mg prior to EN initiation 2) Initiate and titrate EN as follows (see table below):Day 1-2: Goal kcal - 20 kcal/kg. Day 2-3: Goal kcal - 25 kcal/kg. Day 3-5: Goal kcal – final goal rate. (See Calorie Calculator).3) Provide thiamine (100 mg) daily x 5 - 7 days. TABLE A: 1.2 kcal/ml Feed TABLE B: 2 kcal/ml Feed NOTE: GUIDELINE ONLYSlower feed rate progression may be required in the following situations:1) Severe malnourishment. 2) Absence of metabolic stress. 3) Inability to access bloodwork daily. 4) Expected delayed electrolyte replacement. Developed by: J. Greenwood, RD. Critical Care Program – Vancouver Coastal Health Authority. Update 7/4/2010. Used with permission.