Download
1 / 16
170 likes | 339 Views
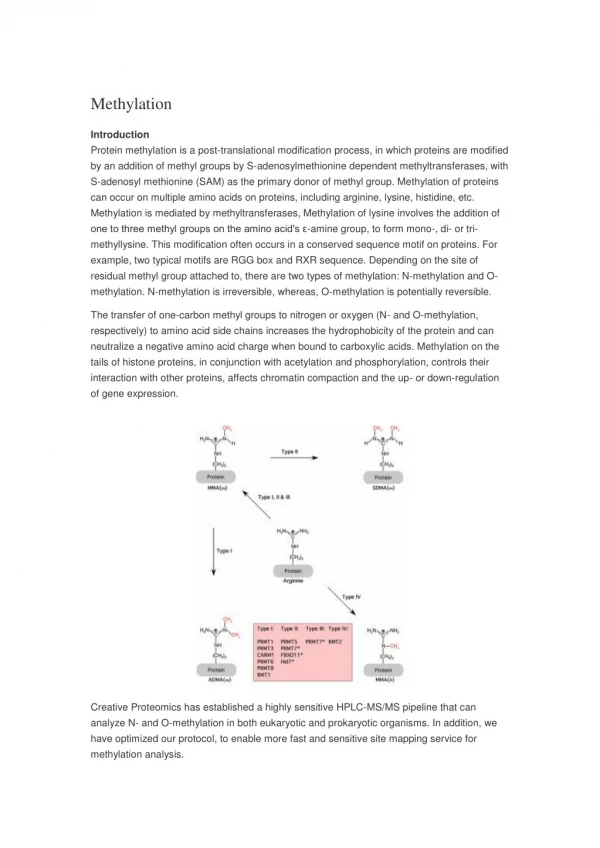
Loss of MLH1 Expression due to Promoter Methylation in Cases Referred for HNPCC. Lorraine Hawkes Kennedy Galton Centre. Hereditary Non-Polyposis Colon Cancer. Inherited pre-disposition to colorectal cancer as well as others - endometrial, ovarian, stomach and small bowel

E N D
Loss of MLH1 Expression due to Promoter Methylation in Cases Referred for HNPCC Lorraine Hawkes Kennedy Galton Centre
Hereditary Non-Polyposis Colon Cancer • Inherited pre-disposition to colorectal cancer as well as others - endometrial, ovarian, stomach and small bowel • Mutations in Mismatch Repair genes – commonly MLH1, MSH2, MSH6, PMS2 • Tumours display Microsatellite Instability • Loss of protein seen on Immunohistochemistry (IHC) • Cancer develops through “adenoma carcinoma sequence”
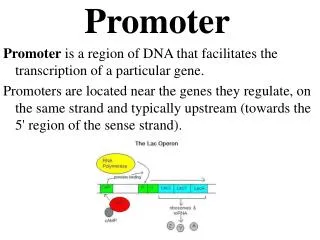
CpG Island Methylator Phenotype (CIMP) • Subset of tumours displaying MSI with wide spread methylation – Toyota et al 1999 • Commonly MLH1 expression lost due to promoter hypermethylation (seen on IHC) • CIMP is seen in ~15% sporadic colorectal cancers • Cancer develops through “serrated pathway” and has a high association with BRAF V600E mutation
CpG Island Methylator Phenotype (CIMP) Categories of tumour: • CIMP high/MSI-H/BRAF V600E • CIMP high/MSI-L/BRAF mutation • CIMP low/MSS or MSI-L/KRAS mutation • CIMP negative/MSS • CIMP negative/MSI-H (HNPCC) Some overlap may be seen
Aims • To set up a routine service to test for promoter hypermethylation of MLH1 in tumours with loss of protein • Retrospectively test tumour samples from HNPCC negative cases with loss of MLH1 and MSI
Tumour sample IHC Loss of MLH1 Loss of MSH2 or MSH6 Normal Result Methylation studies Mutation screen MSI and reporting Positive – Report Negative – Mutation screen Testing Strategy
Methods • ME001B Tumour Suppressor 1 MS-MLPA Kit (MRC Holland) - 41 probes (26 testing for methylation – 2 for MLH1) • ME011 Mismatch Repair kit (released part way through study) - 32 probes (21 testing for methylation – 5 for MLH1)
Results • 45 tumour samples tested • 35 patient blood samples tested (where available) Tumour Results:
Results • Hypermethylation not found in any patient blood samples • 1 sample with low level methylation • 3 of normal patients later found to have variants: - c.2041G>A, p.Ala681Thr (confirmed pathogenic) - c.694G>A p.Gly232Arg (unclassified variant) - c.199G>A. p.Gly67Arg (unclassified variant) • One patient with two different tumours - colon is normal - gall bladder tumour hypermethylated
Normal methylation results and no MLH1 mutation • Mutation in non-coding region of MLH1? • Change of protein/mRNA expression without structural change to the gene? • HNPCC mutation missed by dHPLC? • Non CIMP, non-HNPCC pathway?
Further Work • Set up testing for BRAF V600E mutation • Investigate promoter methylation in patients with loss of MSH6 or MSH2 and no mutation • Patients negative for hypermethylation now to have full gene sequencing • Work on quantifying methylation using Coffalyser programme
Conclusions • MS-MLPA is a useful pre-screen for tumour samples referred for HNPCC, with loss of MLH1 • Reliable • Cost efficient • A significant proportion of samples referred for HNPCC testing are found have loss of MLH1 due to promoter methylation
Acknowledgements • Sam Butler • Stewart Payne • Lindsey Sutherland • Marco Novelli (Histopathology, UCL)