Download
1 / 29
300 likes | 477 Views
Cardiac Disorders. Rachel Hindin, MD Washington University School of Medicine Department of Medical Education Grace Hill Murphy O’Fallon Clinic. Outline. Anatomy Physiology History & physical Diagnostic studies Treatments Medications Percutaneous interventions Devices

E N D
Cardiac Disorders Rachel Hindin, MD Washington University School of Medicine Department of Medical Education Grace Hill Murphy O’Fallon Clinic
Outline • Anatomy • Physiology • History & physical • Diagnostic studies • Treatments • Medications • Percutaneous interventions • Devices • Cardiac disorders • CAD • CHF • Arrhythmias • Valvular disease • Pericarditis
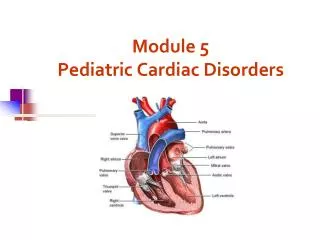
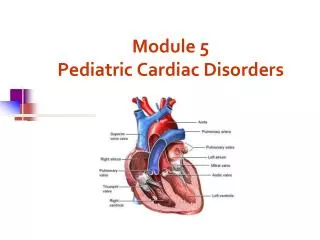
Cardiac Anatomy – Internal • Blood flow • RA • RV • LA • LV
Cardiac Conduction • Electrical conduction • SA node • AV node • Bundle branches • Purkinje fibers
Electrocardiogram • P-wave: atrial contraction • QRS: ventricular contraction
Cardiac Evaluation: History • Chest pain • Palpitations • Shortness of breath • Orthopnea • Paroxysmal nocturnal dyspnea • Edema • Syncope
Cardiac Inspection Jugular venous distension Palpation PMI Thrill/heave Auscultation Rate Rhythm Heart sounds: S1, S2, S3, S4 Murmurs Pulmonary Crackles/rales Abdominal Hepatosplenomegaly Ascites Peripheral Edema Cardiac Evaluation: Physical
Diagnostic Studies • Noninvasive • EKG • Stress test • Echocardiogram • Holter monitor/event monitor • Chest X-ray • Invasive • Cardiac catheterization • EP study
Treatment: Medications • Medications • Beta-blockers – decrease heart rate, cardiac contractility, and stress on arterial wall • Metoprolol, Toprol, Atenolol, Carvedilol • ACE inhibitors – decrease production of vasoconstrictor angiotensin (resulting in vasodilation); exert beneficial effects on cardiac remodeling • Enalapril, Lisinopril, Quinapril, Accupril • Diuretics – increase urine production (decrease amount of water in body) • Lasix • Glycosides – increase cardiac contractility; decrease heart rate • Digoxin/Lanoxin • Statins – decrease production of cholesterol • Lipitor, Zocor, Mevacor, Pravachol • Anti-platelet agents – decrease ability of blood to form clot • Aspirin, Plavix
Treatment: PCI/Devices • Percutaneous Coronary Intervention (PCI) • Angioplasty • Coronary artery stenting • Devices • Pacemaker (PPM) • Automated Internal Cardiac Defibrillator (AICD)
Coronary Artery Disease (CAD) • CAD – focal narrowing of coronary arteries as a result of intimal proliferation of smooth muscle cells and the deposition of lipids (i.e. plaque formation) • Risk factors • Age – gender – cholesterol – smoking – HTN – FMHx – DM • Myocardial ischemia – narrowing of coronary artery prevents increase in coronary blood flow needed to compensate for increased demand (i.e. oxygen demand exceeds oxygen supply) • Myocardial infarction (MI) – necrosis of myocardial tissue due to prolonged ischemia
CAD: Diagnosis • Signs • Signs of vascular disease • Symptoms • Exertional chest pain radiating to left arm/jaw, associated with nausea, diaphoresis, shortness of breath – sx relieved with rest • EKG – localizes general area of active ischemia or old infarction through changes in electrical tracing • Stress test – localizes specific area of active ischemia or old infarction through decreased perfusion • Echocardiogram – visualizes wall motion abnormalities • Catheterization – directly visualizes stenotic and occluded arteries
CAD: Treatment • Medications • Aspirin • Beta-blocker • ACEI • Statin • Procedures • Percutaneous Coronary Intervention • Angioplasty • Coronary artery stenting • CABG
Congestive Heart Failure (CHF) • CHF – inability of heart to pump enough blood to meet oxygen requirements of the body tissues • Systolic vs diastolic dysfunction • Systolic dysfunction – decreased cardiac contractility, resulting in decreased cardiac output • Diastolic dysfunction – decreased ventricular relaxation and impaired filling, resulting in decreased cardiac output • Left- vs right-sided failure • Left – left ventricle fails • Right – right ventricle fails
CHF: Etiology • Ischemic cardiomyopathy • Coronary artery disease/MI • Nonischemic cardiomyopathy • Dilated • Hypertrophic • Restrictive • Idiopathic
Non-ischemic Cardiomyopathies • Dilated • Pathophysiology – decrease in contractility of ventricles (in absence of pressure overload or CAD), leading to loss of cardiac muscle function and CHF • Etiology – EtOH, doxorubicin, endocrinopathies, cobalt/lead, metabolic disorders, prolonged tachycardia • Hypertrophic obstructive • Pathophysiology – hypertrophy of interventricular septum leading to LV outflow obstruction • Etiology - genetic • Restrictive • Pathophysiology – stiffening of myocardial tissue leading to restriction of LV filling and decreased output • Etiology – infiltrative disease (amyloidosis, hemochromatosis, sarcoidosis)
CHF: Diagnosis • Symptoms • Shortness of breath, cough, lower extremity swelling • Signs • Heart murmur, extra heart sounds, displaced PMI, pulmonary rales, jugular venous distension, ascites, lower extremity edema • EKG – visualization of ischemic, infarcted, or hypertrophied regions of heart • CXR – visualization of pulmonary edema and cardiomegaly • Stress test • Echocardiogram – quantification of LV output/systolic function; visualization of impaired cardiac relaxation/diastolic function
CHF: Treatment • Medications • Beta-blocker • ACEI • Diuretic • Glycoside • Devices • AICD
Arrhythmias • Arrhythmias: abnormal cardiac rhythms due to abnormalities in cardiac conduction pathway • Tachyarrhythmias: >100 bpm • Atrial • Ventricular • Bradyarrhythmias: <60 bpm • Sinus • AV nodal • Symptoms • Palpitations, SOB, syncope • Signs • Abnormal rhythm on auscultation • Diagnostic studies • EKG • Holter/event monitor • EP study
Tachyarrhythmias: Atrial • Regular • Sinus tachycardia – increase in sinus rate secondary to other physiologic process • Atrial flutter – increased atrial rate, intermittently but regularly conducted to the ventricles • Irregular • Atrial fibrillation – many irregular impulses begin in and spread through atria and are conducted irregularly to ventricles • Multifocal atrial tachycardia – atrial contraction arising from multiple specific sites in atrium and conducted to ventricles • Treatment • Rate control • Rhythm control • Anti-coagulation
Tachyarrhythmias: Ventricular • Regular • Ventricular tachycardia – ventricle contracts rapidly and regularly, independent of normal atrial rhythm • Irregular • Premature ventricular contractions – ventricle contracts before atrial impulse is received • Ventricular fibrillation – irregular, discoordinate, rapid contraction of ventricle leads to no cardiac output = FATAL • Treatment • Rate control • Defibrillation
Bradyarrhythmias • Sinus node dysfunction • Sinus bradycardia – decreased sinus node rate • Sinus pause – failure of sinus node to put out impulse on time • AV node block – some of impulses generated from sinus node not conducted to the ventricles • Mobitz I/II block – dropped beats • Complete block – no impulses conducted from atria to ventricle (heart rate dependent on spontaneous ventricular contraction) • Treatment • PPM
Valvular Disease • Classification • Stenotic disease • Aortic stenosis • Mitral stenosis • Regurgitant disease • Aortic regurgitation • Mitral regurgitation • Tricuspid regurgitation • Symptoms/signs: CHF sx, arrhythmia sx • Diagnosis: EKG, TTE, CXR, cath • Treatment (varies by dz): diuresis, rate control, increase contractility; valve repair/replacement
Stenotic Disease • Aortic stenosis (AS) • Pathophysiology – pressure overload on LV due to increased pressure needed to pass stenotic valve; results in LV hypertrophy • Etiology – senile calcific AS, bicuspid AoV, rheumatic heart dz • Mitral stenosis (MS) • Pathophysiology – impedes LV filling; results in increased LA pressure, pulmonary congestion, increased RV pressure • Etiology – rheumatic heart dz (female predominance)
Regurgitant Disease • Aortic regurgitation (AR) • Pathophysiology – portion of LV output flows backwards into LV during diastole; results in decreased diastolic BP • Etiology – syphilis, aortic dissection, Marfan’s, collagen vascular dz • Mitral regurgitation (MR) • Pathophysiology – portion of LV output pumped backwards into LA rather than forwards into aorta during systole; results in increased LA pressure and decreased cardiac output • Etiology – rheumatic heart dz, CAD, infective endocarditis, MVP • Tricuspid regurgitation (TR) • Pathophysiology – portion of RV output flows backwards into RA rather than forwards into pulmonary artery during systole; results in systemic venous congestion • Etiology – infective endocarditis, RV failure, rheumatic heart dz
Pericardial Disease • Classification • Acute pericarditis • Pericardial effusion • Cardiac tamponade • Symptoms: chest pain, shortness of breath • Signs: friction rub, distant heart sounds • Diagnosis: EKG, CXR, TTE • Treatment: tx underlying etiology; pericardiocentesis
Acute Pericarditis • Pathophysiology – inflammation of pericardial tissue surrounding heart • Etiology • Viral • Collagen vascular dz • Infectious (TB) • Drug induced (hydralazine, isoniazid) • Malignancy (pulmonary, breast metastases) • Uremia (renal failure) • Complication • Constrictive pericarditis • Diffuse thickening of pericardium in reaction to prior inflammation • Reduced distensibility of cardiac chambers resulting in decreased cardiac output
Pericardial Effusion/Cardiac Tamponade • Pathophysiology • Effusion – inflammation of pericardium causes collection of fluid in pericardial space • Tamponade – effusion develops so rapidly or becomes so large that it compresses heart • Treatment – pericardiocentesis