Download
1 / 15
190 likes | 578 Views
Hepatic encephalopathy/ Portal-systemic encephalopathy /hepatic coma Hepatic encephalopathy is a neuropsychiatric syndrome caused by hepatic insufficiency

E N D
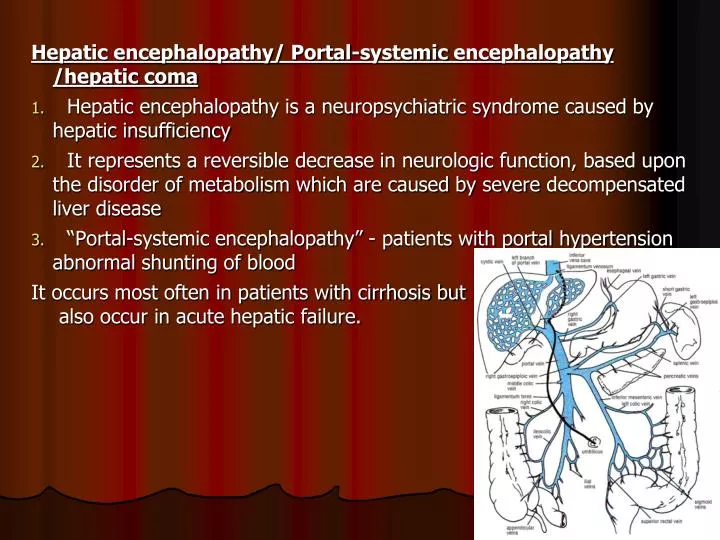
Hepatic encephalopathy/ Portal-systemic encephalopathy /hepatic coma • Hepatic encephalopathy is a neuropsychiatric syndrome caused by hepatic insufficiency • It represents a reversible decrease in neurologic function, based upon the disorder of metabolism which are caused by severe decompensated liver disease • “Portal-systemic encephalopathy” - patients with portal hypertension abnormal shunting of blood It occurs most often in patients with cirrhosis but also occur in acute hepatic failure.
Causes: • Chronic parenchymal liver disease: • Chronic hepatitis: • Cirrhosis. • Fulminating hepatic failure: • Acute viral hepatitis • Drugs • Toxins e.g. Wilson’s Disease, CCL4, Surgical Portal-systemic anastomoses, - portacaval shunts, or Transjugular intrahepatic portal-systemic shunting [TIPS]).
Factors precipitating hepatic encephalopathy: • Metabolic stress • Infection • Electrolyte imbalance, especially hypokalemia; • Dehydration , Renal failure • Diuretic drugs, • Disorders that increase gut protein • GI bleeding • High-protein diet • Nonspecific cerebral depressants • alcohol, sedatives, analgesics
Pathogenesis • Absorbed products – detoxified in Liver • PSS – toxic substances enter systemic circulation - Which are toxic to brain Other factors • Increase sensitivity to GABA (inhibitory neurotransmitter) • Increase circulating levels of endogenous benzodiazepines
Pathogenesis (acute & chronic ) • The basic cause is same in both forms but the mechanism is somewhat different • Diminished detoxification of toxic intestinal nitrogenous compounds Increased in blood NH3 etc Toxic effect on brain Appearance of abnormal amines in systemic circulation Interference with neurotransmission Dr S Chakradhar
Endotoxins of HE • Ammonia • Mercaptans - degradation of methionine in the gut • Phenols • Free fatty acids
Ammonia Production • Small intestine: degradation of glutamine produced NH3 • Large intestine: Breakdown of Urea and proteins by normal flora • Muscles: proportion to muscle work • Kidney: increased production when hypokalemia and diuretic therapy • Liver: detoxified ammonia into urea • Brain can also detoxified ammonia into glutamine
Clinical Features of hepatic encephalopathy: A Disturbance inconsciousness • Disturbances in sleep rhythm. • Impaired memory/ apraxia • Mental confusion. • Apathy. • Drowsiness / Somnolence • Coma.
B. Changes Personality • Childish behavior. • May be aggressive out burst. • Euphoric. • Foetor hepaticus – Foul–smelling breath associated with liver disease due to mercaptans
C Neurological signs: • Flapping tremor / Asterixis (in pre coma). • Exaggerated tendon reflex. • Extensor plantar reflex.
Investigations Diagnosis is usually made clinically • No Pathognomonic liver function abnormality • Elevation of blood ammonia • Hypokalaemia • EEG (Electroencephalogram) • CSF & CT Scan – Normal • Other Routine Investigations - TC, DC, ESR, Hb, Na, k, Urea, Creatinine, Prothrombin time
Differential Diagnosis • Subdural Haematoma • Drug or Alcohol intoxication • Wernicke’s encephalopathy • Hypoglycaemia
Treatment • Hospitalization is mandatory • ABC maintain • Remove the cause & precipitating factors • IV fluid dextrose saline & Inj. Thiamine • Maintenance of fluid, electrolytes & calorie • Diet – Restriction of protein diet • High glucose diet • Avoid constipation – Lactulose 15-20ml X 3 times a day • Antibiotics : • Neomycin • Ampicillin • Metronidazole • Inj. Vitamin K
Mechanism of action of Lactulose: • Osmotic laxative effect. • It reduces pH of colonic content & thereby prevents absorption of NH3. • Incorporates nitrogen into bacteria