Download
1 / 19
190 likes | 362 Views
Investigating the use of Multiple Displacement Amplification (MDA) to amplify nanogram quantities of DNA to use for downstream mutation screening by sequencing and MLPA. Kirsty Manger Nottingham Molecular Genetics. Introduction.

E N D
Investigating the use of Multiple Displacement Amplification (MDA) to amplify nanogram quantities of DNA to use for downstream mutation screening by sequencing and MLPA Kirsty Manger Nottingham Molecular Genetics
Introduction • Often significant amounts of DNA are required in the detection of mutations • e.g BRCA1 and BRCA2. • This may lead to the exhaustion of DNA and prevent further testing. • Improvement in mutation detection techniques have provided an option to rescreen patients with more sensitive techniques.
Project Plan • Investigate the use of MDA for mutation screening by sequencing and MLPA. • Test if MDA provides genome wide amplification without any bias or preference for certain chromosomes or chromosome regions.
Project Plan MDA DNA tested: • Sequencing – BRCA1 and BRCA2 • Southern blotting – DM • MLPA –BMD/DMD • Quantitative fluorescent PCR- BMD/DMD
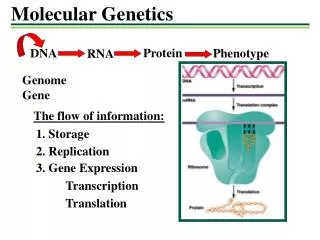
Basis of technique • Random hexamer primers are annealed to denatured DNA. • Strand displacement synthesis at a constant temperature of 30 ºC to produce gDNA products of a high molecular weight (100kb). • Reaction is catalysed by the DNA Polymerase from the Bacteriophage Φ29 -high proof reading capability with error rates one hundred times lower than that of Taq Polymerase.
Previous studies • Genotyping of 45 SNPs on a single microarray showed a >99% agreement between original gDNA and the MDA product* • Pooling of single cell MDA products for STRs and SNP analysis can reduce allele drop out and still produce accurate results • In the absence of DNA template there is occasionally the production of spurious bands on the gel *Lovmar et al Nucleic acids research, 2003, vol.31, No.21
Previous studies • It has been estimated that typically 20-30µg of DNA is produced per 100µl of MDA reaction* • MDA has the potential to provide sufficient amounts of DNA for array-CGH from small amounts of cells if good quality DNA is available** • Uncertainty regarding genomic coverage by MDA and the possibility of amplification bias in different chromosomal regions • The testing of dosage measurements would need to be further validated • Not validated for use in a diagnostic laboratory *Dean et al PNAS Vol99 No.8 5261-5266 2002 ** Lovmar et al Human Mutation 27(7), 603-614,2006
Method Lane 1 = gDNA =0.05µg Lane 2 =MDA product from gDNA = ~1.3µg • The kit used was commercially available from Qiagen – REPLI-g® Mini/.Midi kit • Recommended starting from >10ng of gDNA template preferably with fragments >2kb • Buffers and polymerases added and the reaction takes place at 30ºC overnight • All samples amplified (=53) • Starting concentration = 10ng typically yielded 15µg (in 50µl)
MDA samples MDA controls Results – BRCA sequencing • Four samples previously tested and reported for diagnostic breast cancer screening were selected for MDA • Sequenced 27/79 amplicons in both directions- one required optimising • Sequence quality was high – all mutations/UV/Poly identified • No SNPs found
BRCA1 ex 11b c.1067A>G BRCA1 ex 03 c.102 del T BRCA1 ex 03 WT BRCA1 ex 11b WT Results – BRCA sequencing
1 X 2 3 Results- DM Southern Blots • People unaffected with DM have either a 9Kb, 10kb or a combination of 9+10Kb alleles when digested with EcoRI • 7µg of MDA DNA was digested with EcoRI for 4 hours. • This was run on a 0.8% agarose gel and hybridised with a M10MH-6 probe
Two females previously reported as normal Normal DMD MLPA trace Two males previously reported as normal Male sample reported with a ex3-29 deletion Results – DMD MLPA
Male diagnostic sample reported as a duplication of exons 3-29 Female carrier samples reported as a deletion of ex 45 Results – DMD MLPA • Were the dosage levels being affected by the MDA process? • Was this a problem with the X chromosome? • MLPA for CMT (Chr 17) also gave inconsistent results • Further work was carried out on the DMD patients using the QFPCR used for aneuploidy screening of chromosomes 13, 18 and 21. • 3’DMD multiplex PCR was also tested
QF-PCR Results • Uses the peak heights to determine the ratios between allele sizes. • Samples with trisomies will have skewed allele ratios (2:1 or 1:2) and often three peaks with a 1:1:1 ratio. • No loss of heterozygosity found in MDA samples
QF-PCR Results • The majority of samples had results that agreed with each other in the pre and post MDA samples • For sample 23-4463 there was a discrepancy between the chromosome 13 results • This sample had been reported as a trisomy 21
46 47 48 45 3’DMD dosage multiplex PCR • Male deletions agreed with the gDNA results • Duplications results for males and females were inconclusive
Conclusions • 100% concordant results with sequencing of MDA products for BRCA1 and BRCA2 genes • Limited Southern blotting for DM but results are encouraging • With DMD MLPA the results were inconsistent • Only male deletion patients were apparent with MDA DNA • These were confirmed by 3’DMD dosage multiplex PCR
Conclusions • QFPCR showed it is likely some areas of gDNA are being copied in equal amounts • No evidence of reliable quantitation from MLPA work so far • Recent paper suggesting similar results* • One drawback of the MDA method is that DNA synthesised does not contain methylated cytosines *Iwamoto et alPlosone DEC2007 issue 12 e1306
Acknowledgments • Dr A Sharif • Lewis Darnell • Dr G Cross • All at Nottingham Molecular Genetics