Download
1 / 44
440 likes | 582 Views
ANEMIA CORRECTION IN. CHF. Commonly seen 30% of non hospitalized CHF 50% of hospitalized CHF patients. IN. Associated. Increased mortality Increased morbidity Hospitalization. With.

E N D
ANEMIA CORRECTION IN CHF
Commonly seen 30% of non hospitalized CHF 50% of hospitalized CHF patients IN Associated Increased mortality Increased morbidity Hospitalization With
Iron Therapy in Chronic Heart Failure (CHF) • most common causes of CHF • -coronary artery disease (CAD) • hypertensive heart disease • valve disease
In CHF anemia defined as hemoglobin (Hb) levels < 12g/dl 11 10 9
In CHF, lower Hb values are usually more prevalent in • - older patients ( Low intake of red meat-GIT bleeding) • patients with poor kidney function ( Low EPO) • patients in the more advanced stages of the disease (Elevated cytokines) • - or presenting with co morbidities ( Diabetes)
The pioneering work of Silverberg et al. has raised interest in the role of anemia in CHF Silverberg DS, Wexler D, Blum M et al. The use of subcutaneous erythropoietin and intravenous iron for the treatment of the anemia of severe, resistant congestive heart failure improves cardiac and renal function and functional cardiac class, and markedly reduces hospitalizations. J Am Coll Cardiol 2000;35:1737-1744. Silverberg DS, Wexler D, Sheps D et al. The effect of correction of mild anemia in severe, resistant congestive heart failure using subcutaneous erythropoietin and intravenous iron: a randomized controlled study. J Am Coll Cardiol 2001;37:1775-1780
mechanism of anemia in CHF CHF frequently affects renal function through renal vasoconstriction and renal ischemia, resulting in chronic renal dysfunction and reduced EPO production. renal vasoconstriction EPO
factors contributing to development of anemia in CHF • affecting iron stores (GIT Problems) • Bleeding due to aspirin administration • Polyps – Oesophagitis • Reduced iron absorption resulting from atrophic gastritis • - haemodilution
factors contributing to development of anemia in CHF • Affecting EPO production • Diabetes • EPO producing cells in kidney may be damaged early by glycosylation • -Anti hypertensive medications • It has also been speculated that the use of • ACE inhibitors • Angiotensin Receptor Blocker may inhibit EPO production
Elevated cytokines • TNF α - IL6 • Cause 4 hematological abnormalities • 2 affecting EPO • Reduced EPO production in the kidney • Reduced activity of EPO in the bone marrow • 2 affecting Iron • Hepcidin • induced failure of iron absorbtion from the GIT • induced trapping of iron in iron stores in the macrophages
Impaired EPO production induces anemia, which, in turn, exacerbates CHF. The process may develop into a vicious cycle that Silverberg et al. call The "cardio-renal syndrome"
Erythropoiesis ─ ─ve effect + + Hepcidin Released From liver By IL6 Fas Ag EPO Iron EPO production Apoptosis Pro-inflammatory cytokines (IL-1, TNFα, IL-6, IFNγ) Fe absorption Fe transport Fe availability (EPO-R, Tf, TfR, Ferriportin, DMT-1) ACE inhibitors
factors contribute to the development of iron deficiency in CHF -poor micronutrient supply of diet -intestinal malabsorption secondary to bowel wall edema -blood loss inherent to aspirin use -In CHF patients with chronic kidney failure, proteinuria may further exacerbate iron deficiency -Besides iron deficiency, insufficient micronutrient supply may also affect folate and vitamin B12 stores.
Anemia contribute to Eccentric LVH
Non-Hematopoietic biological effects of EPO Some of these effects are due to the increase in number and activity Of endothelial progenitor cells (EPCs) from the bone marrow Reduce apoptosis of the cardiomyocytes oxidative stress and inflammation fibrosis Prevent hypoxic damage functional impairment of the heart Increase neovascularization Improve endothelial dysfunction wound healing
Effect on smooth muscle tension Eicosanoids influence the state of tension of the smooth muscles. Depending on the impulse that the smooth muscle cells are exposed to, they change from a state of tension to a state of relaxation and vice versa These signaling molecules thereby have a direct effect on important bodily functions, such as bloodpressure regulation breathing intestinal activities.
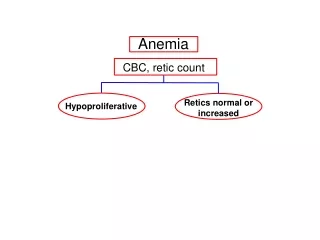
Concepts We check Hemoglobin Ferritin Transferrin Serum transferrin receptors MCH MCV No
What a body needs iron for Hormone formation formation of hormones can only occur if a biochemical impulse for their production is sent. This requires enzymes - substances, also known as catalysts these enzymes need iron to do their job
depression Serotonin an endorphin, is also often referred to as the “happy hormone.” Dopamine Like serotonin, dopamine is called a “happy hormone”
Insomnia Melatonin regulates the functioning of what is known as our inner clock DSIP (Delta Sleep Inducing Peptide) produces the deep sleep, an important sleep phase that is responsible for the quality of our nightly recovery.
Energy production Each body cell contains a large number of mitochondria We consider them our “power plants” and they use adenosine triphosphate (ATP) to produce the necessary chemical cell energy It is the iron-sulfur molecules, which are the central constituents in the cascade of chemical reactions that results in energy being released in the cells
Eicosanoid formation Eicosanoids are our organism’s iron-containing signaling molecules, which directly influence many of our bodily functions a) Effect on smooth muscle tension b) Influence on the stomach c) Effect on the immune system
c) Effect on the immune system: The eicosanoids also include leukotrienes. Those are small acid particles in the white blood cells, which are effective in connection with allergic and inflammatory reactions. It is also the function of leukotrienes to “attract” the body’s antibodies to the site of an infection.
in CHF
Anemia Patient selection • Before considering using Erythropoietin • Evaluate other causes of anemia • (bleeding) • Obtain CBC • Hgb - RBCs count - MCV- MCH • Assess for adequate iron stores • Ferritin 50 ng/ml or more • TS 20% or more
How to assess Iron store Ferritin kits < 10 ng/ml 50 ng/ml 100 ng/ml > 100 ng/ml invalid
Hemoglobin From monitor to Close monitor Step 1 Insert the TEST CARD Step 2 Apply the SAMPLE Step 3 Read the RESULT in 2 min
Anemia Goals of therapy Restore the iron needed for Erythropoiesis & other functions Resolution of sever anemia with target Hb 12 g/dl Reduce need for transfusion and or hospitalization Enhance quality of life
IRON MANAGMENT Energy to live … not just to survive Initiate therapy with IRON Each 1 gm Hgb require 150 mg of bioavilable iron Calculate iron stors by ferritin test Iron stores should be at least 500 mg
erythropoietin Energy to live … not just to survive Initiate therapy with Erythropoietin 50 IU/Kg/W Recheck Hgb every 2 weeks Till goals of therapy achieved
erythropoietin ESA Partial responder Hgb increase less than1gm/dl After 4 weeks Stop Erythropoietin once target Hg Of 12 g/dl achieved check iron stores If iron stores are adequate Increase Epo dose 25%
erythropoietin ESA responder Hgb increase 1-2 gm/dl/month with Hgb still less than 12g/dl Stop Erythropoietin once target Hgb of 12g/dl achieved maintain Epo dose
The Hemoglobin Sweet Spot Risk 100% 50% Hb g/dL 9 11 12 13
Heme iron polypeptide YES Efficient Absorption 23 times greater than iron salts Absorption is through the heme receptors Aong the GIT Compliant Taken with meals Taken with tea &coffee Not affected by Gastric acidity as it Does not need to change to Ferrous-Ferric- Ferrous Quality Made in Sweden
Heme iron polypeptide No Constipation Cramping Heartburn Nausea EFFICIENT NATURAL
Heme iron polypeptide Available in ?
Not affected by gastric acidity Affected by gastric acidity Limited absorption Higher absorption