Download
1 / 60
600 likes | 838 Views
Lower Urinary Tract & Sexual Function Following Pelvic Surgery. “The Vulnerable Pelvis”. Patricia A. Wallace M.D. Assistant Professor, UCIMC Female Pelvic Medicine & Reconstructive Surgery The Incontinence & Support Institute. Objectives. Definitions: Lower urinary tract symptoms (LUTS)

E N D
Lower Urinary Tract & Sexual Function Following Pelvic Surgery “The Vulnerable Pelvis” Patricia A. Wallace M.D.Assistant Professor, UCIMC Female Pelvic Medicine & Reconstructive Surgery The Incontinence & Support Institute
Objectives • Definitions: • Lower urinary tract symptoms (LUTS) • Female sexual dysfunction • Prevalence of LUTS & sexual dysfunction in general population • Pelvic anatomy & vulnerable areas
Objectives • Effects of pelvic surgery • General gyn surgery • Incontinence & prolapse surgery • Surgery for gyn malignancy • Surgery for colorectal disorders • Multidisciplinary approach to surgery & recovery
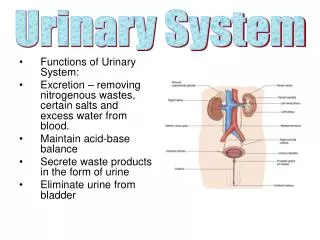
Lower Urinary Tract Symptoms(LUTS) • Symptom-subjective indicator of a change in condition as perceived by patient, caregiver, or partner and may lead to the person seeking health care • Storage symptoms • Urgency, frequency, nocturia, incontinence, abnormal bladder sensation • Voiding symptoms • Slow stream, hesitancy, split stream, intermittent stream • Post micturition symptoms • Postvoid fullness or dribbling
Lower Urinary Tract Symptoms(LUTS) • Symptoms associated with prolapse • Vaginal bulge or pressure • Symptoms associated with intercourse • Dyspareunia, dryness, incontinence • Urinary tract & sexual pain symptoms • Pain in bladder, vulva, vagina, etc
Lower Urinary Tract Symptoms(LUTS) • Frequency >8 voids/24 hrs • Urgency- strong desire to void • Nocturia > 1-2 /nt • Incontinence- (Symptom) Involuntary leakage of urine • Preceded by urgency-Urge • Associated w/increased abdominal pressure-Stress • DetrusorOveractivity- (Sign/Dx) involuntary detrusor contraction, spontaneous or provoked • Idiopathic detrusoroveractivity replaces detrusor instability • Neurogenicdetrusoroveractivity replaces detrusorhyperreflexia The Standardization of Terminology of Lower Urinary Tract Function International Continence Society; Neurourology and Urodynamics 2002
Overactive Bladder • A collection of symptoms consisting of urgency, frequency, nocturia, with and without incontinence • No identifiable pathologic or metabolic condition to explain symptoms
Overactive Bladder & Urinary Incontinence • Approximately 15-17% of population have symptoms of OAB • Incidence increases with age • 38% of women > 65 • 27% of women < 65 • Incidence in institutionalized women > 80% • Associated with poor quality of life, depression • More common than osteoarthritis and diabetes
Prevalence of LUTS • 2863 postmenopausal women • HERS trial • Mean age 66.7 yrs • Baseline questionnaires • Prevalence • Stress incontinence sx- 13% • Urge incontinence sx-14% • Any incontinence sx- 28% • Urge incontinent women voided more frequently during day & night Brown et al. Obstet Gynecol 1999
Prevalence of LUTS • 4103 community dwelling women screened using validated questionnaires • Age 24-84 (mean 56.5) • Prevalence • Stress incontinence 15% • OAB 13% • POP 6% • Anal incontinence 25% • Co-occurrence of mixed sx 69-80% Lawrence. Obstet Gynecol 2008
Risk Factor for LUTS • Pelvic floor disorders • Age • Race • Obesity • Smoking • Childbirth • Urge incontinence/OAB • Increased age • Menopausal status • Diabetes • Urinary tract infection • Prior pelvic surgery • Stress incontinence • Caucasian race • Increased BMI • Higher waist to hip ratio • Parity/mode of delivery • Prolapse • Parity • Mode of delivery • Brown. Obstet Gynecol 1999 • Lawrence. Obstet Gynecol 2008 • Lucacz. Obstet Gynecol 2006 • Dooley Y et al. J Urol 2008 • Fenner D et al. J Urol 2008
Sexual Function vs Dysfunction Highly variable Life cycle & age Sexual response cycle in women Personal distress caused by symptoms related to sexual response cycle
BLENDED INTIMACY-BASED SEXUAL DRIVE-BASED CYCLES Emotional Intimacy Motivates the sexually neutral woman Emotional & Physical Satisfaction To find/ be responsive to “Spontaneous sexual drive hunger” Sexual Stimuli Arousal & Sexual Desire Psychological and biological factors govern “arousability” Sexual Arousal Basson R. Obstet Gynecol 2001; 98:350
Prevalence of Sexual Dysfunction Affects 25%-43% of women 1 Multidimensional and multicausal combining biological, psychological, and interpersonal factors 1,2 Physically and emotionally distressing Increases with age 1 1.Bancroft j. Arch Sex Behav. 2003; In Press 2. Laumann EO, et al. JAMA. 1999;281:537
Risk Factors for Sexual Dysfunction Aging and menopause Chronic medical conditions: DM, HTN, Depression, CAD Pelvic surgery* Neurological disorders: MS, epilepsy, paralysis Endocrine disorders: Addisons disease, hypothyroidism Medications: SSRIs, antihypertensives, steroids, statins, other psychotropics Infection: STDs or condyloma
Female Sexual Dysfunction • Sexual desire disorders • Hypoactive sexual desire disorder • Sexual aversion disorder • Sexual arousal disorder • Orgasmic disorder • Sexual pain disorders • Dyspareunia • Vaginismus • Noncoital sexual pain disorder *International Consensus Development Conference on Female Sexual Dysfunction.Basson R, et al. J Urol. 2000;163:888-93.
LUTS & Sexual Dysfunction • 25-50% women with pelvic floor disorders • Most common • Decreased libido • Dyspareunia • Decreased orgasm • Urinary incontinence independently associated with worse sexual function Handa. AJOG 2004
The Vulnerable Pelvis Superior hypogastric plexus Inferior hypogastric plexus Pudendal nerve & sacral nerve roots
General Gynecology • El-Touky. J Obstet Gynecol 2004 • Kluviers. J Minim Invasive Gynecol 2007 • Gutl. J Psychosom Obstet Gynecol 2002 • Kupperman et al. Obstet Gynecol 2005 • Hysterectomy- any route • Mild improvement in LUTS 1,2 • Improvement in sexual function 3 • Postmenopausal status, severity of gynecologic complaints, & preop frequency predictors of sexual outcomes • Abdominal scar/pain short term impact • Supracervical & abdominal hysterectomy-similar outcomes 4
Oophorectomy • Teplin. Obstet Gynecol 2007 • Aziz. Maturitas 2005 • Premenopausal woman • Worse body image • Poor sleep • Decreased overall quality of life SF-36 • No difference in sexual scores, urinary complaints • At 2 years-Equivalent! • Improvement in gynecologic condition & postoperative well-being
Incontinence Surgery & LUTS • Burch • Postoperative retention • >30 days rare • Usual catheter 7-10 days • OAB 7-27% postop • Enterocele & rectocele 7-26% • Slings • Pubovaginal slings • Postop voiding disorders 12.8% (3-37%) • OAB/UI 7% (3-30%) • Retropubic • Voiding dysfunction/retention 1-3% • OAB/UI 2-50% (includes de novo & preexisting) • Erosion 3%-7% • Transobturator • Groin pain & abscess <1-3%
Incontinence Surgery & Sexual Function • Limited research • Short term1 • Improvement in sexual function scores • Correlates with improvement in incontinence • No change in frequency, desire, arousal, orgasm & satisfaction • Retropubicvstransobturator sling • Improvement in sexual life2 • ?increased risk of sexual pain 3-14%3 • Rogers. AJOG 2006 3. Latthe. BJOG 2007 • Pace. J Sex Med 2008
Prolapse Surgery • Postoperative voiding dysfunction variable • 10-30% risk of recurrence of prolapse • Sexual dysfunction • Rectocele repair (5-37% dyspareunia) • Abdominal apical repair1 • More women sexually active • Decreased sx interfere w/sex & avoidance of sex • Less pain • Vaginal apical repair vs abdominal repair2 • Dyspareunia at 1 yr 34% vs 7%, 3 yrs 32% vs 11% • Handa. AJOG 2007 • Arya. SGS 2008
Prolapse Surgery with Mesh Posterior Mesh Kit Anterior Mesh Kit
Prolapse Repair with Mesh 8 papers/presentations at AUGS Oct 2007 10 papers/ presentations at SGS April 2008 Erosion rates 2-13% Reoperation rates for erosion, fistula, or pain 20% Dyspareunia 38-41%
SGS Guidelines for Use of Graft In Prolapse Surgery • Systematic review • Medline 1950-2007 • Publications on comparative studies using vaginal grafts • Adverse events of non-comparative studies
How to GRADE the evidence… • Quality of Evidence • High-more research unlikely to change confidence in effect • Moderate-more research likely to change confidence in effect & may change estimate of effect • Low-very likely to change confidence in effect & likely change estimate of effect • Very Low- any estimate of effect is uncertain • Recommendations • Strong- high quality evidence &/or other considerations support strong recommendation • Moderate-high or moderate evidence &/or other considerations support moderate recommendations • Weak-low or very low evidence support weak recommendation, based mostly on expert opinion
SGS Recommendations • Anterior Compartment • Biologic & Absorbable synthetic- Native tissue repairs are appropriate when compared to biologic graft (weak) • Synthetic-Non-absorbable mesh may improve anatomic outcomes, but trade-offs with risk of adverse events (weak) • Apical/Multiple Compartments • No comparative studies to guide any recommendation on the use of biologic, absorbable, & non-absorbable synthetic graft in multiple compartment repair when compared to native tissue repair (weak) • Posterior Compartment • Biologic & Absorbable synthetic- Native tissue repairs are appropriate when compared to biologic graft (weak) • Synthetic- No comparative studies to guideuse of non-absorbable mesh when compared to native tissue repair (weak) SGS Proposed Clinical Guidelines on Vagina Graft Use 2008
Surgery for Gynecologic Malignancy • Recognized risk of injury to genitourinary tract • Radical nature of surgery • Pelvic radiation & chemotherapy • Limited literature • Mostly retrospective • Primarily cervical malignancy • Evaluated postoperative or therapy
Effects of Radical Hysterectomy • Hypertonicity-early & transient • Voiding dysfunction • Abdominal straining • Decreased compliance • Stress incontinence • Detrusoroveractivity
Gynecologic Malignancy & LUTS • Farquharson et al 1986 • 15% baseline report urinary incontinence • Stress incontinence more common in surgery alone group-26% (10-52%) • Urgency, mixed incontinence >RT group • 63% incidence of incontinence following radical hysterectomy + radiation • No difference in bladder sensation • RH + RT less bladder compliance
Gynecologic Malignancy & LUTS • Lin et al 2000 • 210 women w/cervical CA plan RH • Preoperative urodynamics • Mean age 49 • 42% menopausal w/o HRT • 17% had NORMAL preopurodynamics • 83% at least one type of LUTD • 73% storage dysfcn • 51% urinary incontinence (37% stress, DO 8%, mixed 6%) • No difference in age, parity, or stage
Gynecologic Malignancy & Sexual Function • Retrospective & limited to postoperative evaluation • Interruption in sexual activity common leading up to diagnosis • Surgery impacts frequency of intercourse & dyspareunia • Radiation more effect locally • Most common effects: • Loss of desire, sensation, & increased pain • Different cancers pose different problems
Gynecologic Malignancy & Sexual Function • 148 women w/gyn malignancies • S/p surgery, RT +/-chemo • Validated questionnaires • Sexually active • 19/41(46%)endometrial • 19/35(51%) cervical • 20/30(66%) ovarian • 74% lack of desire • 40% dyspareunia • 51 cervical ca survivors • Validated questionnaires • No difference • Interest • Sexual pleasure • Survivors • Increased pain, dryness • More likely to use HRT • Trend towards dec arousal & orgasm Wenzel. Gyn Onc 2005 Thranov. Gyn Onc 1993
Colorectal Surgery Sigmoid & rectal cancer patients most vulnerable Similar risk to adjacent organs & nerves Most studies retrospective or descriptive, done postoperatively Men studied more than women Combined LUTS & sexual function Improvement in outcomes with evolution of nerve sparing techniques
Prevalence of Male & Female Sexual Dysfunction is High Following Surgery for Rectal Cancer • 223 pts s/p curative colorectal cancer surgery • 81 women, 99 men • Validated questionnaires • FSFI • IIEF • EORTC QLQ-C30 & QLQ-CR38 • 25/81 (31%) sexually active • 20 yrs younger than non-active grp • 20 yrs younger at time of surgery • 19/81 (23%) reported surgery made sex life worse • 73% Desire problems (28% A vs 54% NA) • 68% Arousal problems (20% A vs 37% NA) • 75% Orgasm problems (24% A vs 44% NA) • 100% Dyspareunia (36% A vs 56%NA) Hendren et al Ann Surg 2005