Download
1 / 26
260 likes | 466 Views
Case 428- 57 year old man with cough and shortness of breath. History.

E N D
Case 428- 57 year old man with cough and shortness of breath
History • A 57-year-old male presented to the emergency department because of a change in his persistent cough and noticeable shortness of breath over the past several days. He has had a chronic cough productive of mucoid sputum for more than 10 years. At least once per year he experiences episodes of acute bronchitis that requires treatment. Antibiotic therapy results in gradual improvement. Approximately 3 weeks ago he noted slightly increasing amounts of purulent looking sputum in the early morning. There have been streaks of blood in the sputum after coughing
More history • The patient works for a construction company and has lived in Omaha since he got out of the army 35 years ago. He has not traveled out of the country. He has smoked 2 packs of cigarettes daily since 17-years-old. He admits to drinking a case of beer a week for years. He denies homosexuality or injection drug use and has not had relations with commercial sex workers. His last chest x-ray was taken about a year before when he was admitted to the Omaha VA Medical Center for “asthma”. His long time private physician recently retired. He has lost weight during the past few months. He thinks about 12 pounds.
Thin, older appearing than age, man in no acute distress. • Vitals: Temp 98° F, pulse 88/min, B.P. 135/80, Resp 16. • HEENT: Conjunctive not icteric, PERRLA, Teeth in poor repair, not thrush. • Neck: Enlarged firm, but not fixed, supraclavicular lymph node of the right side. • Chest: Area of bronchial breath sounds and whispered pectoriloquy anteriorly beneath the right clavicle and in the right supraclavicular fossa. The trachea was shifted to the right. Scattered coarse rhonchi were heard throughout the remainder of both lung fields and expiration was prolonged. • Heart: Regular rate and rhythm. No murmurs heard. • Abdomen: Liver span was 15 cm. The spleen was not palpable. Bowel sounds normal.
Extremities: Definite clubbing of the fingers was present. Skin: numerous spider angiomata were seen over the upper thorax, shoulders, neck and face. Palmer erythema was noted, but no asterixis was present. Neuro: Oriented x3, cranial nerves I-XII grossly intact. No focal neurologic defects were observed. Write a problem list and initial differential. Based on this what further tests or procedures would you order at this time?
Chest Xray • PA and lateral chest x-ray reveals a density in the right lower lobe consistent with partial atelectasis of the lobe. The right diaphragm was elevated. Attempts to locate previous radiographs were unsuccessful. CT scanning of the chest with contrast showed mediastinal nodes in the right paratracheal and subcarinal groups whose diameters were more than 2 cm. The right lower lobe bronchus could not be traced from its take off from the right main bronchus suggesting an obstructive lesion. There was volume loss in the right lower lobe that confirmed the atelectasis, but an inflammatory process could not be excluded. Views of the adrenals and liver failed to show any metastatic nodules.
Labs • Hgb: 15 gm/dL • Hct: 45 % • RBC: 5.25 x 106 uL • WBC: 10,000 x 103 uL • Platelets: 205 x 103 uL • Na: 138 mMol/L • K: 4.5 mMol/L • CO2 (HCO3): 20.0 mMol/L • Cl: 98 mMol/L • BUN: 18 mg/dL • Creatinine: 1.0 mg/dL • Glucose: 110 mg/dL The patient was admitted.
What is your differential now? • What would you do now? • Why was the skin tests given and explain the findings. Skin tests were applied with IPPD and Candida antigens. The IPPD test was negative at 2 days. The Candida test was reactive. Three early morning sputa were examined for AFB by Ziehl-Neelsen and fluorchrome stains and were negative. These were also cultured for bacteria, AFB and Fungal organisms and examined for malignant cells.
Additional Laboratory Test Results Were Available The Next Day • Calcium: 12 mg/dL • Uric acid: 7.5 mg/dL • AST: 80 Iu/L • ALT: 60 Iu/L • Bilirubin: 1.1 mg/dL • Alk phosphate: 110 Iu/L
Sputum cytology from this patient showing the malignant squamous cells
Fiberoptic bronchoscopy was then performed with topical anesthesia. The orifice of the right lower lobe bronchus was completely occluded by a friable endobronchial mass. Cytologic material and biopsies were taken. Material was also obtained to culture.
The biopsy (available the next day) showed: Microscopic section of the bronchial mucosa showing the transition from normal mucosa to areas of atypia and carcinoma in situ
Microscopic sections of the tumor showing well-differentiated squamous cell carcinoma (note keratin pearls).
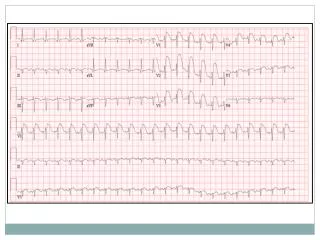
Describe the biopsy findings? • What is the diagnosis and what management strategy would you begin? ECG showed nonspecific changes. Pulmonary function studies revealed severe airway obstruction with FEV, of only 0.7 L despite bronchodilator therapy. Quantitative lung scanning showed that the right lung contributed 40% of his overall lung function. (A right pneumectomy would leave the patient with a FEV, of less than 0.5L). Mediastinoscopy showed metastatic carcinoma in the right paratracheal and subcarinal groups
What is the probable stage of the tumor and how would you treat him? What is the final problem list and differential? The patient was deemed not a candidate for surgery and was given palliative care and died several months later. Autopsy was performed and the pertinet findings shown:
Gross photos of this man's lungs at autopsy. Note the central location of the tumor, the peribronchial extension, and the extension into the mediastinal lymph nodes. The tumor involves the carina making resection impossible. Note the centrilobular emphysema. This tumor was obstructive and there is atelectasis distal to the tumor mass
Note the central location of the tumor, the peribronchial extension, and the extension into the mediastinal lymph nodes. The tumor involves the carina making resection impossible. Note the centrilobular emphysema. This tumor was obstructive and there is atelectasis distal to the tumor
Microscopic section of the bronchial mucosa showing the transition from normal mucosa to areas of atypia and carcinoma in situ
Other areas of the lung showed: Severe centriacinar emphsema
The patient also had moderate fatty change (steatosis) with early cirrhosis of the liver
Briefly classify the primary neoplasms of the lung. What is the relationship of smoking to each of the tumor types? • Discuss some local (i.e. intrathoracic) complications of lung tumors. • What is a paraneoplastic syndrome? Give examples. Which one(s) did this man have? • If this patient had grey-black discoloration of the axillae, what would this be called and possibly indicate?
Describe some classic paraneoplastic syndromes. An example of acanthosis nigricans
What is the prognosis of a patient with this type of tumor? How are pulmonary tumors staged and what is this patient’s stage?