Download
1 / 36
360 likes | 370 Views
Explore the changes in UK deceased donor kidney transplantation, assess discarded kidneys, and propose strategies for better kidney utilisation. Learn about improving organ offering, data analysis, and decision-making support. Acknowledge the collaboration of healthcare professionals in addressing utilisation challenges. ###

E N D
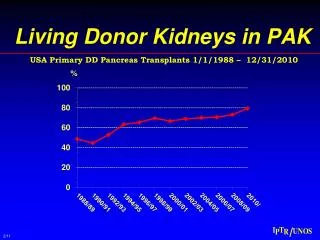
Can we improve deceased donor kidney utilisation? Chris Callaghan National Clinical Lead for Abdominal Organ Utilisation, NHSBT Consultant Transplant Surgeon, Guy’s Hospital Renal Transplant Services Meeting, March 2016
Introduction • How has UK deceased donor kidney transplantation changed? • Can we improve kidney utilisation? • If so, how?
Variation in appetite for risk High risk Standard risk
Transplantation pathway DBD donors Organs consented? Organs transplanted? Organs suitable? Organs accepted? Organs retrieved? SNOD SNOD/ Tx centre Transplant centres NORS teams/ tx centres Transplant centres DCD donors Organs consented? Organs suitable? Organs accepted? Organs retrieved? Organs transplanted? SNOD SNOD/ Tx centre Transplant centres NORS teams/ tx centres Transplant centres Death in timeframe?
Discard rate of retrieved kidneys from deceased donors, Apr 2009 – 31 Mar 2014
Deceased donor kidneys retrieved but not transplanted – reasons for non-use
NHSBT service evaluation:discarded donor kidneys Shruti Mittal, Chris Callaghan On behalf of NHSBT
Methods • 30 consecutive discarded kidneys; April 2015 • Assessed at Guy’s Hospital • EOS core donor data form (CIT ignored) • Macroscopic appearance • Histology: Remuzzi/Karpinski score (0-12) • Usable / probably usable / not usable
Kidney 5 & 6 (113734) • 72F DCD, intracranial haemorrhage, weight 71kg • PMH: Hypertension • UO 8105 ml/24 hours, creatinine 55 K-score 5 and 6
Kidney 11 (113929) • 67M DCD, intracranial haemorrhage, weight 104kg • PMH: haematuria, atrial flutter • UO 1520 ml/24 hours, creatinine 100 K-score 3 +
Kidney 10 (113900) • 72M DBD, hypoxic brain injury (anaphylaxis), weight 90kg • PMH: hypertension, renal calculi, • UO 3790 ml/24 hours, creatinine 97 K-score 4
Analysis of discarded kidneys • 10 (32%) were considered usable • Equates to 75 discarded kidneys in 2014/15 • Are discarded kidneys really usable?
Improving organ utilisation • General • Engagement with colleagues to identify barriers to utilisation • Recent survey to surgeons
Improving organ utilisation • General • Engagement with colleagues to identify barriers to utilisation • Raise awareness of utilisation issues
Improving organ utilisation • General • Engagement with colleagues to identify barriers to utilisation • Raise awareness of utilisation issues • Provide an evidence-base to enable better decision-making
Improving organ utilisation • General • Engagement with colleagues to identify barriers to utilisation • Raise awareness of utilisation issues • Provide an evidence-base to enable better decision-making • Improve data on utilisation practices to centres
Improving organ utilisation • Kidney • Analyses of discarded kidneys • Better data on reasons for organ decline / discard • More efficient organ offering / allocation policies for marginal kidneys • Minimising cold time before kidney inspection • Provision of organ images with fast-track offers • Use of warm perfusion technology to enable viability assessment
Conclusions • Rapid changes in donor type and demographics • Transplant outcomes are stable • Variation in clinical decision-making • Likely that usable organs are being discarded • Multiple approaches needed to improve organ utilisation and support clinicians to make difficult decisions
Acknowledgements • Lisa Bradbury • Rachel Johnson • Sarah Hosgood • Mike Nicholson • ShrutiMittal • Sally Rushton • James Neuberger