Download
1 / 1
10 likes | 170 Views
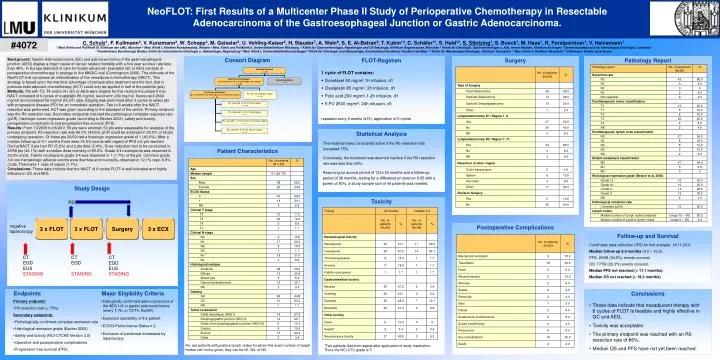
NeoFLOT: First Results of a Multicenter Phase II Study of Perioperative Chemotherapy in Resectable Adenocarcinoma of the Gastroesophageal Junction or Gastric Adenocarcinoma. #4072.

E N D
NeoFLOT: First Results of a Multicenter Phase II Study of Perioperative Chemotherapy in Resectable Adenocarcinoma of the Gastroesophageal Junction or Gastric Adenocarcinoma. #4072 C. Schulz1, F. Kullmann2, V. Kunzmann3, W. Schepp4, M. Geissler5, U. Vehling-Kaiser6, H. Stauder7, A. Wein8, S. E. Al-Batran9, T. Kubin10, C. Schäfer11, S. Held12, S. Stintzing1, S. Boeck1, M. Haas1, R. Forstpointner1, V. Heinemann1 1 Med. Klinik und Poliklinik III, Klinikum der LMU, München 2 Med. Klinik I, Kliniken Nordoberpfalz, Weiden 3 Med. Klinik und Poliklinik II, Universitätsklinikum Würzburg, 4 Klinik für Gastroenterologie, Hepatologie und GI-Onkologie, Klinikum Bogenhausen, München 5 Klinik für Onkologie, Gastroenterologie u. Allg. Innere Medizin, Klinikum Esslingen 6 Gemeinschaftspraxis für Hämatologie/Onkologie, Landshut 7 Krankenhaus Barmherzige Brüder, Klinik für Internistische Onkologie u. Hämatologie, Regensburg 8 Med. Klinik I, Universitätsklinikum Erlangen 9 Klinik für Onkologie und Hämatologie, Krankenhaus Nordwest, Frankfurt am Main 10 Klinik für Hämatologie/Onkologie, Klinikum Traunstein 11 Med. Klinik II, Klinikum Neumarkt 12 ClinAssess GmbH, Leverkusen Consort Diagram Background: Gastric Adenocarcinoma (GC) and adenocarcinoma of the gastroesophageal junction (AEG) display a major cause of cancer related mortality with a five year survival rate less than 40%. In Europe standard of care for locally advanced resectable GC or AEG consists of perioperative chemotherapy in analogy to the MAGIC-trial (Cunningham 2006). The rationale of the NeoFLOT-trial comprises an intensification of the neoadjuvant chemotherapy (NACT). This strategy is based upon the manifest advantage of perioperative treatment and the fact, that in previous trials adjuvant chemotherapy (ACT) could only be applied in half of the patients (pts). Methods: Pts with T3, T4 and/or N+ GC or AEG were eligible for this multicentric phase II trial. NACT consisted of 6 cycles of oxaliplatin 85 mg/m2, leucovorin 200 mg/m2, fluorouracil 2600 mg/m2 and docetaxel 50 mg/m2 (FLOT) q2w. Staging was performed after 3 cycles to select pts with progressive disease (PD) for an immediate operation. Two to 6 weeks after the NACT, resection was performed. ACT was given according to the standard of the centre. Primary endpoint was the R0-resection rate. Secondary endpoints included the pathological complete response rate (pCR), histologic tumor regression grade (according to Becker 2003), safety and toxicity, perioperative complications and progression free survival (PFS). Results: From 10/2009 to 06/2011 59 pts were enrolled, 50 pts were assessable for analysis of the primary endpoint. R0-resection rate was 86.0% (43/50). pCR could be achieved in 20.0% of all pts undergoing operation. Of these pts 20/50 had a histologic regression grade of 1 (40.0%). After a median follow-up of 9.1 monthsthere were 34.5% events with regard of PFS not yet reached. During NACT 3 pts had PD (5.2%) and 2 pts died (3.4%). Dose reduction had to be conducted in 25/58 pts (43.1%) with a median dose intensity of 89.2%. Grade 3/4 neutropenia was observed in 29.3% of pts. Febrile neutropenia grade 3/4 was observed in 1 (1.7%) of the pts. Common grade 3/4 non-hematologic adverse events were diarrhea and mucositis, observed in 12.1% resp. 6.9% of pts. There was 1 case of sepsis (1.7%). Conclusions: These data indicate that the NACT of 6 cycles FLOT is well-tolerated and highly effective in GC and AEG. FLOT-Regimen Surgery Pathology Report Patients Enrolled n = 59 • 1 cycle of FLOT contains: • Docetaxel 50 mg/m2,1h infusion, d1 • Oxaliplatin 85 mg/m2, 2h infusion, d1 • Folic acid 200 mg/m2,1-2h infusion, d1 • 5-FU 2600 mg/m2, 24h infusion, d1 • repeated every 2 weeks (d15), application of 6 cycles Intent-to-treat Analysis (pts allocated for 6 x chemothrapy and surgery) n = 58 Screening failure n =1 Pts. did not undergo surgery n = 8 Per Protocol Analysis (pts. completed chemotherapy and underwent surgery) n = 50 Pts. received 6 x FLOT and surgery n = 46 Pts. received 5 x FLOT and surgery n = 1 Pts. received 1 x FLOT and 5 x FLO and surgery n = 1 Pts. received 6 x FLOT and no surgeryn = 2 Statistical Analysis The treatment was considered active if the R0-resection rate exceeded 75%. Conversely, the treatment was deemed inactive if the R0-resection rate was less than 60%. Assuming an accrual period of 12 to 24 months and a follow-up period of 36 months, testing for a difference on level α= 0.05 with a power of 80%, a study sample size of 44 patients was needed. Patient Characteristics Study Design Toxicity PD 3 x FLOT 3 x FLOT Surgery 3 x ECX negative laparoscopy Postoperative Complications Follow-up and Survival Cutoff date data collection CRO for first analysis: 18.11.2011 Median follow-up 9.0 months (0.0 – 16.2). PFS: 20/58 (34.5%) events occured. OS: 17/58 (29.3%) events occured. Median PFS not reached (> 17.1 months). Median OS not reached (> 19.2 months). CT EGD EUS STAGING CT EGD STAGING CT EGD EUS STAGING Endpoints Major Eligibility Criteria Conclusions • Primary endpoint: • R0 resection rate (> 75%) • Secondary endpoints: • Pathologically confirmed complete remission rate • Histological remission grade (Becker 2003) • Safety and toxicity (NCI-CTCAE Version 3.0) • Operative and postoperative complications • Progression free survival (PFS) • Histogically confirmed adenocarcinoma of the AEG I-III or gastric adenocarcinoma (every T, N+ or T3/T4, Nx,M0). • Expected operability of the patient. • ECOG-Performance-Status ≤ 2. • Exclusion of peritoneal metastasis by laparoscopy. • These data indicate that neoadjuvant therapy with6 cycles of FLOT is feasible and highly effective in GC and AEG. • Toxicity was acceptable. • The primary endpoint was reached with an R0-resection rate of 86%. • Median OS and PFS have not yet been reached. • N+ are patients with positive lymph nodes for whom the exact number of lymph • nodes can not be given, they can be N1, N2, or N3. *Two patients died from sepsis after application of study medication. There the NCI-CTC grade is 5.