Download
1 / 19
210 likes | 403 Views
Health Inequalities in the New Public Health System. 28 th February 2012 Dr Jessica Allen Deputy Director Marmot Review Team Institute of Health Equity UCL. New Public Health System. Move to local authorities Money? Focus – health services or SDH? Leadership CCGs?

E N D
Health Inequalities in the New Public Health System 28th February 2012 Dr Jessica Allen Deputy Director Marmot Review Team Institute of Health Equity UCL
New Public Health System • Move to local authorities • Money? • Focus – health services or SDH? • Leadership • CCGs? • Population focus? – registration • Funding? • Health inequalities? • NHS Workforce?
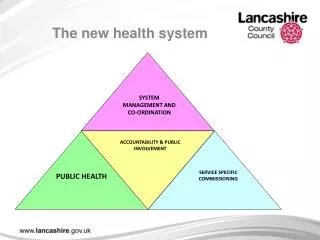
Health and Wellbeing Throughout Life • Empowering Local Government and Communities • Taking a life course approach • Giving every child the best start in life • Making work pay • Designing communities for active aging and sustainability. • Collaborative working with business and the voluntary sector • A new public health system with strong local and national leadership.
Approach for new public health system tackling health inequalities
Fair Society, Healthy Lives (The Marmot Review) • Health inequalities are not inevitable or immutable • Health inequalities result from social inequalities - ‘causes of the causes’ – the social determinants • Focusing solely on most disadvantaged will not be sufficient - need ‘proportionate universalism’ • Reducing health inequalities vital to economy - cost of inaction
Strategic Drivers: 6 key policy objectives of Fair Society, Healthy Lives. • Give every child the best start in life • Enable all children, young people and adults to maximise their capabilities and have control over their lives • Create fair employment and good work for all • Ensure healthy standard of living for all • Create and develop healthy and sustainable places and communities • Strengthen the role and impact of ill health prevention
Policy Development and delivery – all levels • Cross government and cross-sectoral • Proportionate universal • Health equity in all policies • International, national and local – multi levelled approach • Partnership working • Involving communities • Public health leadership
Prevention and Regulation E.g. Smoking ban in public places. Standard of Living E.g. Tackling debt problems. Employment and Work E.g. Address stress at work. Communities and Places E.g. Reducing environmental inequalities. Delivery system E.g. BLT Strategy E.g. Advertising campaigns Delivery system E.g. Feeling good about where you live E.g. Free NRT Education and Skill Development E.g. Reduce the number of NEETs. E.g. Weight management programmes Delivery system E.g. Swansea and Wrexham E.g. 5-a-day campaign X E.g. Stop smoking programmes E.g. School educational programmes Delivery system E.g. Birmingham Brighter Futures Downstream interventions Equity E.g. Reducing population groups’ differences in PPHCs Early Years E.g. Increase children and family services. Framework
The risk of fuel poverty according to household income, England 2009
Educational attainment is a predictor of health outcomes. • Higher educational attainment is associated with healthier behaviour. • There is a gradient in limiting illness by level of educational attainment. • There is a gradient in mortality by educational attainment. Education and Skills
Local Government • Complex, disparate and diverse systems of Local Government. • Focus on needs of local population and place. • Differing capacities to orchestrate action to address the social determinants of health.
How? • Whole System Leadership. • Involving elected members • Public health in all sectors - Links with other sector • Areas of focus – early years, transport, planning, education, fuel poverty etc. • Co-production • Increasing participation and empowering communities.
Creating conditions in which individuals and communities have control over their health and lives and participate fully in society.