Download
1 / 37
370 likes | 596 Views
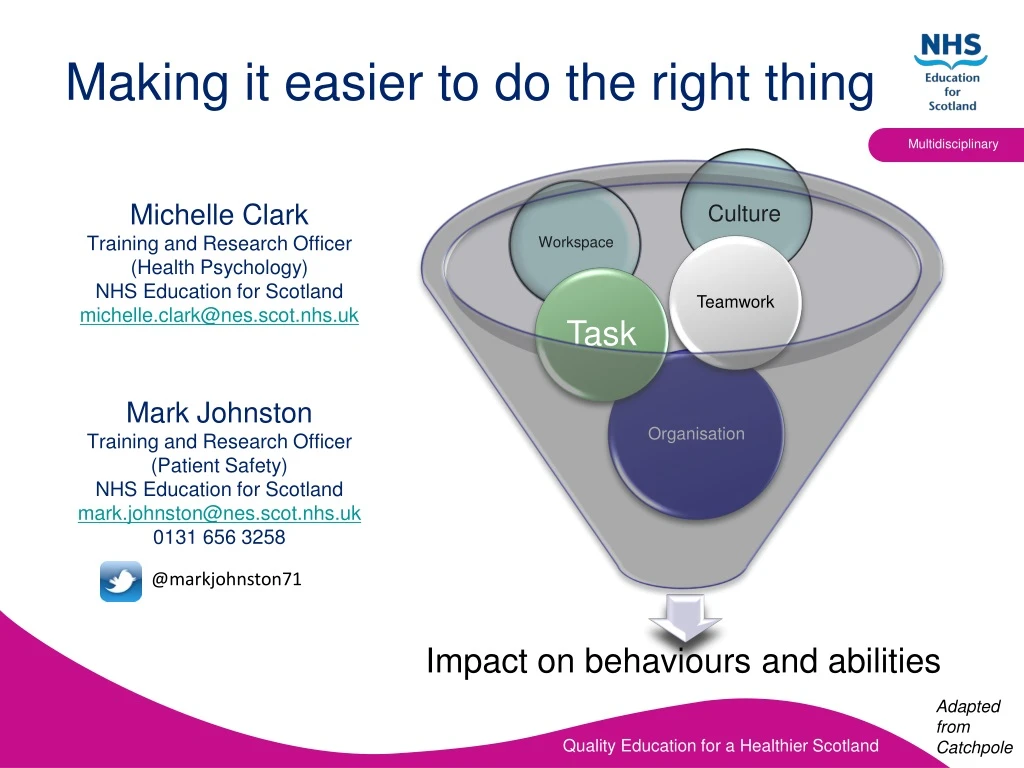
Making it easier to do the right thing. Michelle Clark Training and Research Officer (Health Psychology) NHS Education for Scotland michelle.clark@nes.scot.nhs.uk Mark Johnston Training and Research Officer (Patient Safety) NHS Education for Scotland mark.johnston@nes.scot.nhs.uk

E N D
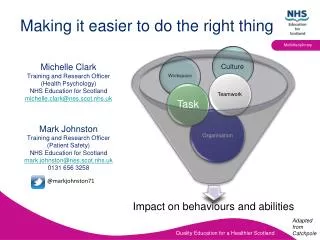
Making it easier to do the right thing Michelle Clark Training and Research Officer (Health Psychology) NHS Education for Scotland michelle.clark@nes.scot.nhs.uk Mark Johnston Training and Research Officer (Patient Safety) NHS Education for Scotland mark.johnston@nes.scot.nhs.uk 0131 656 3258 Culture Workspace @markjohnston71 Impact on behaviours and abilities Adapted from Catchpole
Human Factors case study – Hand hygiene behaviours of final year medical students
Pilot study – what we did • Final year medical students at University of • Dundee Medical School • Mixed methodology Qualitative (n=9) Based on students’ final year ‘ward simulation exercise’ assessment video ‘Self-explanatory’ interview Categorical content analysis using HF & Health Psychology theory frameworks. Quantitative (n=30) Questionnaire assessing • Predictors of HH behaviour • Barriers & levers to HH behaviour
Results – Questionnaire Predictors of behaviour Attitudes Normative beliefs Behaviour intentions Behaviour Perceived behavioural control Theory of Planned Behaviour (Ajzen & Fishbein, 1980)
Results – QuantitativeBarriers & Levers(Theoretical Domains Framework (TDF) Michie et al 2008) • The higher the number of barriers, the less HH behaviour is carried out • Compared TDF domains based on levels of compliance (high or low) ** ** Mean scores
Results – Qualitative‘Self-explanatory’ interview Observable HH behaviour low (despite high self reported HH) Individual factors Positive impact • Attitudes & beliefs (capabilities & consequences of HH) • Motivation • Negative impact • Stress & anxiety • Human cognition & memory (mental load, dual processing, primacy effects Task related factors Negative Impact Multiple tasks • Switching between multiple patients • Changing symptom presentation • Problem solving nature of tasks Environment factors Positive Impact • Multiple gel bottles • Prominent location • Negative Impact • Layout of ward • Layout of paperwork/forms.
HH Pilot study (cautious) conclusions • Clear intention-behaviour gap (self report & observed HH behaviour) • Cognitive factors & beliefs about capabilities are barriers to HH (in this group) • Making several decisions within a high pressure situation lead to high cognitive load which negatively affects memory – automaticity not achieved • Need to believe you are capable of performing HH • Attitudes towards HH & Social influence (especially from influential staff members) can predict HH behaviour • Primacy effect evident in practice of WHO 5 moments, but not recency effect (forgot moments 4&5).
Implications... • Teaching of Hand Hygiene behaviour • Impact of stress/anxiety and cognitive load on HH behaviour & make behaviour automatic even in stressful situations • Other prompts to remind & encourage habits at more of the WHO moments.
So, some thoughts on why…? • Bad people? • Error occurs due to Systemic and Systemic induced Individual failure • Negligence is not the same as error, both may result in harm
Why do we make mistakes? Sometimes we do the wrong thing, consciously and sub-consciously
Driving 100 mph illegal for all Borderline Tolerated Conditions of Use Driving 75 mph – the ‘illegal-illegal’ space (for almost all of us!) Individual Pressures Individual Autonomy Normalisation of Deviance Driving 64 mph -the illegal- normal space Perceived Vulnerability VERY UNSAFE SPACE The posted speed limit is 60 mph- the ‘legal’ space Accident Belief in Systems- guidelines <1% 5% 50% 80% 100% percent of drivers PERFORMANCE Adapted from Rene Amalberti
Human FactorsA common language “Enhancing clinical performance through an understanding of the effects of teamwork, tasks, equipment, workspace, culture and organisation on human behaviour and abilities and application of that knowledge in clinical settings” (Catchpole 2010) “Making it easy to do the right thing” (Bromiley 2011) • Individual Worker • -Cognitive skills • Situation awareness • Decision making • - Personal resources • Management of stress • Management of fatigue Organisational/ Management -Safety Culture -Managers’ Leadership -Organisation communication Work/Environment -Work environment and hazards (ergonomics) Workgroup/Team -Teamwork structures & processes -Team Leadership (Flin, Patey 2012)
The first lesson in reducing harm is the realisation that we will and do make mistakes ‘It’s the downside of having a brain!’ Reason
Multi-tasking - Our lazy brains would rather default to system 1 2 x 2 = 4…System 1 17 x 379 = 6443…System 2. Kahneman 2012
Card suit change game • Groups of three • 1 Person deals cards, turning them face up in rapid succession and estimates the passing of time • If you deal all the cards deal them again • 1 person estimates the passing of time with no aid and counts the number of times the cards change suit. • 1 person times the activity using an aid and then focuses only on recording the suit changes • When told to finish, separately record the time and number of suit changes and compare your results
Where can we start? “Making it easy to do the right thing” (Bromiley 2011) Work/Environment -Work environment and hazards (ergonomics) (Flin, Patey 2012)
‘We cannot change the condition of those who do the work, but we can change the conditions within which they work’ Reason J. BMJ. 2000 March 18; 320(7237): 768–770.
Everyone, everywhere, every time Good human factors design in health care accommodates everyone Not just the calm, rested experienced healthcare worker But also the inexperienced health-care worker who might be stressed, fatigued and rushing.
Where can we start? “Making it easy to do the right thing” (Bromiley 2011) Organisational/ Management -Safety Culture -Managers’ Leadership -Organisation communication (Flin, Patey 2012)
‘We cannot change the condition of those who do the work, but we can change the culture within which they work’
What is your culture? Nurses Managers Doctors Silo working?
Do we pay attention to the Swiss cheese or do we blame? Our learned behaviour is to blame an individual Society, peers, media Imperfect System Our colleagues, ourselves?
Where can we start? “Making it easy to do the right thing” (Bromiley 2011) Workgroup/Team -Teamwork -Team Leadership (Flin, Patey 2012)
Lessons for Leadership inchanging culture Culture change and continual improvement come from what leaders do, through their commitment, encouragement, compassion and modelling of appropriate behaviours. Berwick Report 2013
Where can we start? “Making it easy to do the right thing” (Bromiley 2011) Workgroup/Team Structures & processes (Flin, Patey 2012)
Examples in healthcare… Prescribing and dispensing Hand-over/hand-off information Movement of patients Order of tests Preparation of medication If all of the processes associated with these tasks make sense and become easier for the ‘human’ to comply with, then patient safety will improve.
Making it easier to do the right thingPDSA example: Christopher Toilet training Aim: Christopher to urinate into the toilet bowl 100% of the time by 30th June 2010.
Example: DSA Do Christopher thought the demonstration amusing and ignored it Study 0% compliance with the new process 0% reliability level Act Seek out ideas, develop new test cycle.
Example: next PDSA cycle A Human Factors approach! http://www.amazon.co.uk/toilet-training-target-stickers-Happeedays/dp/B002GZAWUK/ref=pd_sim_by_3
Making it easier to do the right thing Michelle Clark Training and Research Officer (Health Psychology) NHS Education for Scotland michelle.clark@nes.scot.nhs.uk Mark Johnston Training and Research Officer (Patient Safety) NHS Education for Scotland mark.johnston@nes.scot.nhs.uk 0131 656 3258 Culture Workspace @markjohnston71 Impact on behaviours and abilities Adapted from Catchpole