Download
1 / 43
430 likes | 777 Views
Wound Care: Where do we go from here?. Jesse M. Cantu, RN, BSN, CWS, FACCWS April 20, 2012 San Antonio, TX. Disease Management (Wound Care Management). Evidence Based Best Practices Standards of Care Positive Outcomes Cost Containment Evolution of Dressings Summary. Wounds. Types

E N D
Wound Care:Where do we go from here? Jesse M. Cantu, RN, BSN, CWS, FACCWS April 20, 2012 San Antonio, TX
Disease Management(Wound Care Management) • Evidence Based • Best Practices • Standards of Care • Positive Outcomes • Cost Containment • Evolution of Dressings • Summary
Wounds • Types • Acute • Chronic • Closure • Phases of Wound Healing
Wounds • Acute wound • Planned / unplanned event • Healing proceeds in an orderly and timely fashion • Examples: • Surgical • Abrasion / laceration
Acute Wound • Surgical incision
Wounds • Chronic wound • Exists two weeks or longer • Does not proceed through normal healing process • Examples: • Pressure ulcers • Diabetic / neuropathic ulcers
Chronic Wound • Pressure ulcer
Chronic Wound • Venous ulcer
Chronic Wound • Post-operative dehisced wound
Wound Closure • Primary intention • Delayed primary • Secondary intention
Evidence Based / Best Practice • Randomized control trials • Protocols (NPUAP, WOCN, Canadian guidelines, AHCPR) • Moist Wound Healing (George Winters) • Wound Bed Preparation (Vincent Falanga)
The Building Blocks of the Foundation for Wound Care Debride Moisture Off-Load Topicals
SUCCESSFUL WOUND CARE NEGATIVE PRESSURE THERAPY BIOLOGIC DRESSINGS SILVER DRESSINGS GROWTH FACTORS BIOENGINEERED TISSUES HYPERBARICS Debride Moisture Off-Load Topicals
Best Practices • Evidence Based • Wound Bed Preparation
Wound Bed PreparationWhat Does It Mean? Originally • Debridement Fibrotic Tissue Hyperkeratotic Rim
Today “…a very comprehensive approach aimed at reducing edema and exudate, eliminating or reducing the bacterial burden and, importantly, correcting the abnormalities … contributing to impaired healing.” Vincent Falanga , MD Professor, Boston University School of Medicine Wound Bed PreparationWhat Does It Mean?
Other Voices…. “Think of it as removing various ‘burdens’ from the wound and the patient.” • Exudate • Bacteria • Necrotic/cellular debris Elizabeth A. Ayello, PhD, RN & Janet Cuddigan, PhD RN
Standards of Care • NPUAP • WOCN • AHCPR • Canadian Guidelines
Positive Outcomes • Wound Assessment at each dressing change
Cost Containment • Wet to Dry Dressings (Gauze and Saline) • Frequent dressing changes • Moist Wound Healing (George Winters 1961) • Active Wound Healing (NPWT, Hyperbarics)
Evolution of Dressings • Debridement • Maintain a moist wound environment • Reduce bacteria load • Prolong dressing interval changes • Stem cell technology
Summary • Wound management not wound care • Need to jump start nonhealing or slow wounds • Adequate assessment, debridement, and wound irrigation based on Best Practices, Evidence based, Standards of Care, Positive Outcomes, and Cost containment • Case studies
Wound Care as Wound Management • Properly treated wounds create the ideal win-win situation by decreasing hospitalizations, promoting wound healing in the home, improving quality of life, and improving patients’ sense of independence and well being.
Other Voices…. Wound Bed Preparation is “the management of a wound in order to accelerate endogenous healing or to facilitate the effectiveness of other therapeutic measures.” Schultz G, Sibbald G, Falanga V, et al:Wound bed preparation: A systematic approach to wound management.Wound Rep Regen 2003
What’s Needed to Heal a Diabetic Neuropathic Ulceration? Control of Diabetes and General Health Adequate Diet Blood Supply Absence of Infection Regular Debridement Offloading of Pressure Moist Healing Environment
Common Methods to “Off-Load” the Foot Total Contact Casts Custom Splints Therapeutic Shoes Removable Cast Walkers
So what is this going to cost me? A lot less than traditional care…
“Incidence, Outcomes, and Cost of Foot Ulcers in Patients with Diabetes” • What is the cost of a new foot ulcer, not previously treated? • $27,987 over a two year period! Ramsey, Reiber, et al. Diabetes Care, Mar 1999 – Univ of Washington
1. Benefits of a Closed Environment • Moisture Balance • Reduction of Nosocomial Infections • Prevents patient interaction with the wound
2. Promotes Perfusion • Replacement of fibrinous tissue with granulation tissue • Filling deficits in wounds • Wound constriction • Promotes granulation tissue formation Dompmartin A, et al J Wound Care 2004 June
Why do we keep a wound moist? Promotes rapid migration of epidermal cells across the wound bed Promotes perfusion
Why do we keep a wound moist? Promotes rapid migration of epidermal cells across the wound bed Promotes perfusion Barrier against environmental contamination
Benefits of Using Negative Pressure Therapy as an Adjunct 70 patients with chronic, non-healing wounds treated with VAC following skin grafts 100 % of the grafts healed in an average of 48 days • Carson SN, Overall K, Lee-Jahshan S, Travis E.Ostomy Wound Manage. 2004 March
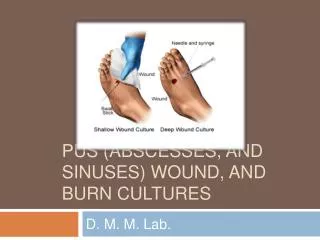
Escalating Bacterial Loads • Contamination – Presence of nonreplicating microorganisms in the wound • Colonization – Presence of nonreplicating microorganisms adhering to the wound, NOT causing injury to the host • Critically Colonized – Bacteria cause a delay in wound healing • Infection Local to Systemic – Presence of replicating microorganisms in wound and presence of injury to the host BA C T E R I A L L O A D Ayello and Cuddigan, 2003
Wound Bed Preparation:Combining Topicals with NPWT Control of: • Contamination, colonization and critical colonization to optimize the wound bed • Odor