Download
1 / 69
740 likes | 1.01k Views
Influenza viruses. Dr Edward Wright wrighte@westminster.ac.uk. Key features of influenza viruses. Orthomyxovirus ss segmented RNA genome 8 segments 5 of the 8 segments in SO-H1N1 A were from swine influenza Lipid envelope with matrix

E N D
Influenza viruses Dr Edward Wright wrighte@westminster.ac.uk
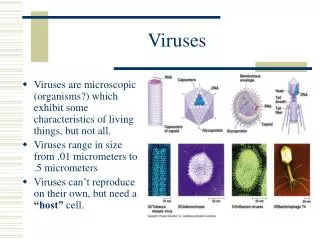
Key features of influenza viruses • Orthomyxovirus • ss segmented RNA genome • 8 segments • 5of the 8 segments in SO-H1N1 A were from swine influenza • Lipid envelope with matrix • Proteins project through the envelope: M2, haemagglutinin (H or HA) and neuraminidase (N or NA) • HA contains 2 polypeptides, HA1 + HA2 concerned with fusion with host cell • HA1 is especially variable • NA is an enzyme cleaving sialic acid, has several functions, most importantly virion release
Influenza subtypes 3 types – antigenic differences in nucleocapsid proteins • Type A • moderate to severe illness • epidemics every 2-3 years • humans and other animals (birds and pigs) • affects all age groups • Type B • milder epidemics • every 4-6 years • humans only, primarily children • Type C • rarely reported in humans • no epidemics
Influenza A + human disease • WHO describes each new isolate as follows: • A/Chicken/Hong Kong/317/01 (H5N1) • Subtype/host of origin/geographical origin/sequential isolate number/year of isolation (H+N type)
The Genome of Influenza A Virus Figure 11.17
The key advantage of a segmented genome is that it facilitates recombination between two strains coinfecting the same cell. New strain can evade the immune system.
The flu virus has no geometric capsid. RNA genome is loosely contained by a shell of matrix proteins. Influenza Virus Structure • RNA segments are coated with nucleocapsid proteins (NPs). • Two major envelope proteins: • - Neuraminidase (NA) • - Hemagglutinin (HA)
Classical influenza • Sudden onset of fever, chills, headache, myalgia and anorexia • Respiratory symptoms may be associated with both URT + LRT infection, often with dry cough • Symptoms may vary with age, with adults more likely to have the systemic effects • Short incubation period of 1-4 days but long convalescent period of 1-2 weeks
Complications • Viral pneumonia may rapidly be fatal • Bacterial pneumonia due to 2o infection • Risk of such complications increases with age and with underlying disease • Sometimes adults are most at risk • Depending on strain: high case fatalities
Diagnosis • Throat swab and vial culture - 3-10 days • Serology – 3 days • PCR – 5 hours More later…
Influenza entry • Sub-categorised on the basis of membrane glycoprotein subtypes: • Haemagglutinin • Viral binding / entry, 18 types differentiated serologically • Neuraminidase • Infection, viral exit, 11 types differentiated serologically • Current human subtypes in circulation – H1N1, H3N2, H1N2 • Host immune response is directed primarily against HA and NA moieties – limit spread and neutralise infectivity respectively
Haemagglutinin (HA) Responsible for infectious entry of influenza into cells by binding to sialic acid receptor on glycolipids and glycoproteins on the surface of lung epithelial cells Name from the property of agglutinating RBCs Entry: through receptor-mediated endocytosis + low-pH-induced fusion from within acidic endosomes Most important surface antigen (neutralising antibodies) It is glycosylated (may help virus to shield antigenic sites from Nabs) Cleaved by cellular protease into 2 subunits: HA1: receptor binding HA2: membrane fusion activity Avian/Human viruses: HA has different cellular receptor specificity (2,3 vs 2,6 linkage)
Cell receptors for influenza virus • Receptor: sialic acid (a family of 9-carbon monosaccharide) • Sialic acids are present on termini of oligosaccharides on cell surface. • Ligand: haemagglutinin Sialic acid Galactose Sialic acid Galactose 9 2 6 9 2 3 SAa2,6Gal SAa2,3Gal Human HA receptor Avian HA receptor
Neuraminidase (NA) • NA: cleaves the sialic acid receptor to release progeny virus from infected cell surface • NA: role in entry also? • NA: target for antiviral drugs (zanamivir+ oseltamivir). • Sialic acid analogues: inhibit the release of progeny virus from infected cells
The haemagglutinin envelope protein attaches to a host cell by binding to a sialic acid receptor protein The virion is taken up by endocytosis. - acidification induces a conformational change Fusion of envelope and the host membrane - contents of the virion are released into the cytoplasm Influenza entry (2)
Viral (–) strand RNA are uncoated and enter the nucleus Influenza mRNA synthesis is primed by capped RNA fragments cleaved from host mRNA Viral mRNA return to cytoplasm for translation Genomic RNA synthesis is primed by NP (+) strand RNA is synthesised by prepackaged RNA-RNA pol, which then uses it as a template for (–) RNA strands These are packaged in newly made nucleocapsid proteins (NPs) and exported to the cytoplasm. Influenza virus replication
Capsid assembly occurs in the cytoplasm. Envelope proteins are synthesised at the ER, where they are glycosylated by host enzymes and transferred to the Golgi for export to the cell membrane. At the membrane, the packaged (–) RNA segments are enveloped by host membrane containing the envelope proteins. Mature virions then bud out of the cell membrane. Influenza virus replication (2)
Animation: Influenza Virus Replication Influenza Virus Replication
Seasonal epidemics vs pandemic • Seasonal epidemic: • 5 to 20% of general population infected • Nursing home attack rates of up to 60% • 85% of flu-related deaths in ages > 65 • Yearly vaccine made against circulating strains • Pandemic • Novel virus to which population has little or no immunity • Virus that is pathogenic and virulent in humans • Virus must be capable of sustained person-to-person transmission • No vaccine
Antigenic Drift and Shift • Antigenic properties altered by: • Antigenic DRIFT: accumulation of mutations in antigenic epitopes of viral antigens • Evolutionary, immunological & drug pressure • Antigenic SHIFT: new HA subtype from recombination • Genetic reassortment between viruses
Antigenic shift • Shift results from large changes in viral genome, producing new combinations of HA + NA • Genetic reassortment between 2 parental viruses has been demonstrated in the lab • Coinfection might enable this to happen in a human or other animal host • Might see a very different virus appearing without warning; no-one would be immune! • Such a virus could spread rapidly through human populations, resulting in a PANDEMIC
Antigenic Drift and Shift (2) • A (+B) can do both • C can only drift • Changes in HA + NA profiles, reflecting changes in coding RNA • Instability of viral RNA during replication
Genetic reassortment between human and avian influenza A viruses gave rise to 2 human pandemics: • 1918: Spanish flu (H1N1) entirely avian, killed 20-50 million • 1957: Asian H2N2 (Av/Hu reassortant) • 1968: HK H3N2 (Av/Hu reassortant), killed >1.5 million • Avian flu that threatens new pandemic is H5N1 (1997, 2003) • 641 cases • 380 deaths • In 2013 – H7N9 in China • 134 cases • 44 deaths • Also risk from “swine flu-like” H1N1 (2009)
Avian influenza • Reservoir of influenza A viruses: wild birds • Avian viruses: cross species barrier to humans and pigs • Result: influenza is a non-eradicable disease • Pandemic preparedness: surveillance of influenza in birds, pigs and humans required
New pandemic threats? H5N1, H1N1 & H7N9
1918 Spanish flu’ H1N1 1957 Asian flu’ H2N2 1968 Hong Kong flu’ H3N2 1977 Red (Russian) flu’ H1N1 Different antigenic strains except 1977 Not clear why H1N1 reappeared Pandemics of the 20th century (have occurred before 20thC but no reliable scientific records)
1918 pandemic(virus re-investigated 2005) • Spanish flu: March 1918-June 1920 • Infected 500 million (1/3 population) and killed 50 million • Many deaths due to secondary bacterial pneumonia • Unusually severe, more deaths in “healthy” persons, theory of over-reactive immune response (“cytokine storm”) increased severity and death • Avian origin • Genome has been sequenced from human tissue but virus was never isolated • Geographical origin is ‘unknown’ – best called 1918 influenza, not Spanish!
1918 pandemic (2) • Spread in 3 waves: Europe, Asia, N America: ~ 50 million died during 1918-1920 • Clearly a sudden appearance of a new virus: no-one was immune! • High mortality • Combination of effective transmission and high pathogenicity: function of its HA + NA profile • High mortality in the children and young adults • No antibiotics to treat secondary bacterial infections
A big worry! • Could an apparently novel strain suddenly appear (as in 1918) to cause a similar pandemic? • Require a virus that can both readily be transmitted from man to man and able to cause severe disease
Recently, we have had 3 candidates: • H5N1 avian influenza virus • H1N1 swine-origin ‘flu virus • H7N9 avian influenza virus
Avian “bird flu”H5N1 - epidemiology • H5N1 bird flu is an avian disease, risk factor for humans handling sick birds • Numerous outbreaks in poultry resulting in large scale culling of domestic flocks to limit disease spread and minimise threat to humans • From 2007-2010 there were 26 outbreaks of H5N1 bird flu that resulted in human infections, 236 cases in infection and 136 deaths (58%) • 59%of people infected with H5N1 bird flu died but little evidence virus is transmitted from human to human • In 2010 there were 48 human cases. Egypt, Vietnam and Bangladesh reported most cases. 83% were in people <40y. 50% died. Exposure to sick or dead poultry in 77% of cases. Still no evidence of sustained human to human transmission. • Since January 2011 there have been 125 (59%) cases of H5N1 in humans, mostly in Egypt
Avian “bird flu”H5N1 – molecular biology • Humans SA2,6Gal receptors are present in upper respiratory tract and SA2,3Gal in lower RT • May explain why avian flu is inefficiently transmitted from person-to-person • Conversion from SA2,3Gal to SA2,6Gal is one of the changes that bird flu must undergo before it can replicate efficiently in humans & cause a new pandemic • Using flu isolates from birds and humans, researchers have found that two HA mutations enough to allow H5N1 bird flu to recognise human receptor SA2,6Gal: • Glnto Arg (192) • Asnto Lys (183) • For H2 (1957) and H3 (1968) pandemic viruses changes to 226 and 228 allowed avian flu to recognise human receptor • While most transmission to humans handling sick birds is limiting the concern about bird flu is adaptation in an infected person to transmission between people
For aerosol spread virus needs to: Replicate in URT – N182K/Q222L/G224S Replicate to high titre – E627K/D701N Release as a single particle – N/A Following passage - Q222L, G224S, E627K, H103Y & T156A
In the UK: H5N1 • Bernard Matthews turkeys in Suffolk in early 2007 • Association with Hungary, virus probably brought in infected meat • Outbreak contained by culling 100,000 birds • No prosecutions; compensation!
Cumulative number of confirmed human cases for avian influenza A(H5N1) reported to WHO, 2003-2013 Total number of cases includes number of deaths WHO reports only laboratory cases All dates refer to onset of illness Source: WHO/GIP, data in HQ as of 08 October 2013
Avian vaccines • Only inactivated ones can be legally used • Activated ones exist and are known to be used illegally • Risk of using activated forms – reassortment to produce a novel and highly pathogenic virus in vaccinated birds
Vaccine strategies against H5N1 influenza • Highly pathogenic H5N1 viruses: kill chicken embryos – propagation of these viruses in eggs = low yields. • Modify these viruses for efficient growth in eggs: reverse genetics (replace multibasic cleavage site) • H5N1 vaccines: low immunogenicity – use of adjuvants, MF59, AS03 • Adjuvantedvaccines: induce broader immune responses (new clades/subclades) Subbarao, 2007 PLoS Pathogens
H5N1 human vaccine • Prepandemic & pandemic preparedness • Undergoing clinical trials • Various inactivated vaccines stockpiled • Baxter, Novartis, Sanofi Pasteur, GSK… • Current status and progress of prepandemic and pandemic influenza vaccine development. Leroux-RoelsI, Leroux-RoelsG Expert Rev Vaccines 2009;8:401-23
Swine flu (or swine-origin H1N1 influenza A) was first reported in March 2009 in Mexico • New strain of H1N1 influenza, arising from a quadruple reassortment • Declared a pandemic in June 2009, WHO raised pandemic alert to 6 (scale 1-6). Officially over by August 2010. • Deadly pandemic failed to materialise • More contagious than seasonal H1N1 • Generally caused a mild illness • Targets younger age group (1918?) • WHO: - 375,000 lab confirmed cases • - 14,000 deaths globally • WHO EU: • - 59,000 cases • - 193 deaths
Pandemic H1N1 in UK • Imported from Mexico or US in 2009 • UK and Ireland were hard hit: Mexico is an important holiday destination • Began to appear in late April/early May • Then transmission in households + schools – some school closures • First death reported 14 June 2009 • This was the first wave of transmission and its peak in July was associated with schools
Pandemic H1N1 in UK (2) • Second wave started when schools returned in autumn and peaked in October • This is the start of the typical flu season • It was the prevailing strain of influenza being transmitted and replaced the predicted seasonal strains
Pandemic H1N1 in UK (3) • Younger people were most likely to be affected • Severe disease and deaths most common in those aged UNDER 65 years old • Those with underlying disease were no more likely to catch disease but were more likely to be hospitalised or die • Overall case fatality rate: 0.4% • NOT A SEVERE DISEASE in the healthy!