Download
1 / 40
440 likes | 713 Views
Learnings from Study Group on Interval Censored Data. DSBS Nytårskur 14 Jan 2010. Study group and litterature What is interval censoring Analysis Methods Graphical presentation Software Examples. Study Group.

E N D
Learnings from Study Group on Interval Censored Data DSBS Nytårskur 14 Jan 2010
Studygroup and litterature • What is interval censoring • AnalysisMethods • Graphicalpresentation • Software • Examples
Study Group • Genmab: Kristian Winfeld, Birgitte Rønn, Wan Hui Ong Clausen, Kim Knudsen, Kamilla Begtrup • Novo Nordisk: Mette Suntum • (Lundbeck: Ole Lemmecke, Nycomed: Henrik Andersen) • Spring 2008-Authumn 2008
Litterature • Book by Jianguo Sun: The analysis of Interval-censoredFailure Time Data • Draft book manuscript by Philip Hougaard: Analysis of –interval-CensoredSurvival Data • HalinaFrydman and Michael Szarek, Non-parametricestimation in a Markov ”illness-death” process from interval censored observations with missing intermediate transition status, Biometrics, 2008, 65, 143-151 and Biostat Research Report
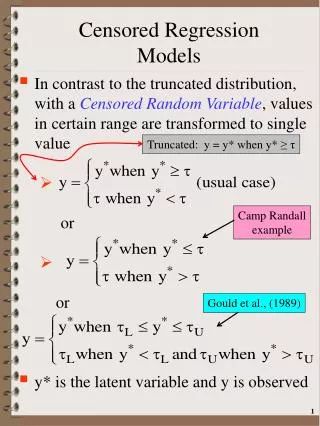
Interval censored data • T failure time • T interval censored if T ∈ (L,R] • R=∞ corresponds to right-censored data
Types of Interval Censoring • Case I interval-censored failure time data/current status data • Observations either right or left censored • T ∈ (L,R] where either L=0 or R=∞ • Case II interval-censored failure time data • T ∈ (L,R] with at least some L and R belonging to(0,∞) • Doubly censored failure time data. • T=S-X where X and S two related events, X≤S and both are interval censored • Most common type of doubly censored data is when S is only right censored • Example: AIDS data • Panel count data/multivariate data • The event can happen multiple times • Only knows the number of occurrences between two time points • Example: recurrence rate of tumor at multiple locations
The situation in oncology trials • Wish to evaluate Progression-free Survival (PFS), i.e., time to death or progression of disease • Progression of disease evaluated by physical examination and CT-scan
300 mg Infusion Infusions Response Evaluation Follow-up Contact Example: Effect of Ofatumumab in patients with Follicular Lymphoma Treatment Follow-up Extended Follow-up Period Period Period 8 infusions 1000 mg N=86 Randomization 500 mg N=31 Scr 0 8 3 6 9 12 18 24 3 4 5 Weeks Months Years Visits
FDA cancer endpoints guideline “We recommend assigning the progression date to the earliest time when any progression is observed without prior missing assessments and censoring at the date when the last radiological assessment determined a lack of progression”.
Interval censoring • The values of the survivor function can only be estimated at the endpoints of the intervals generated by (Li, Ri]. • Sufficient only to consider intervals with positive probablity mass – the Peto-Turnbull intervals
Example • Intervals : (1,2], (1,4], (3,6], and (5,6] • CorrespondingPeto-Turnbullestimates: (1,2], (3,4] and (5,6] • Intervals withprobabilitymasszero: (2,3] and (4,5] are not (L,R] intervals
Methods • Parametric models • Relative easy. The likelihood can be written explicitely
Semi-Paramteric model • Estimation can be done via the Newton-Raphson algorithm but unstable estimation problems can occur in situations with large number of different observation time points. • When no exact failure times are observed, Hypothesis testing can be performed via the Wald test or a Score test. • For the general case, the asymptotic properties of the estimates are not fully explored. • Ordering of the events is unknown – i.e., impossible to separate the effect of covariates from the effect of time.
NPMLE for Type II censored data • Studycontains of n independent subjects from survivalfunctionS(t). • g • g • Likelihood: • MaximiseLs(p) withrespect to p, with ∑pj=1 are the ordereddistinct time points of {Li,Ri} αij = indicator for time point sj in (Li,Ri]
NPMLE for type II censored data • Estimation done via iteration – several approaches available (Turnbull, ICM, EMICM, etc). • convergence can be difficult • global maximum not guaranteed. • Estimation problem can be simplified by finding the intervals with positive probability mass. (Peto-Turnbull intervals). • If enough exact failure times are available or if the inspection process is non-random the NPMLE can have n1/2-convergence rate and as. normal dist. Otherwise, order is only n1/3 and asymptotic distribution is not normal.
GeneralizedLog-rank Test for type II censored data Notation: = ML estimator of common Surv funct under H0 are the ordereddistinct time points of {Li,Ri} αij = indicator for time point sj in (Li,Ri] δi = indicator for Ti not right censored, I(Ri≤sm) ρij = indicator for Ti right censored and subject i still at risk at sj-, I(δi = 0, Li≥ sj)
Generalizedlog-rank test for case II censored data Under H0: overall estimate of numbersfailing at sj is: The number at risk at sj is estimated as: = number of failures at sjorlater + number right censored and at risk at time sj
Case II interval censored dataGeneralizedlog-rank test Principle:Log-rank test = sum of observed minus expected no. of events Covariance matrix, Vr for Urestimated by multiple imputation. Then
How to draw survival curve when S(t) only estimated at endpoints of the intervals (Li, Ri] ? The estimatedsurvivalcurve
Software • Parametric models: R, SAS PROC LIFEREG or NLMIX • Semi-parametric models: SAS PROC NLMIX except when data includes exact observation times or many distinct timepoints.
Software, NPMLE Estimation • Splus: Estimates in KM procedure (Turnbull’s self-consistency algorithm) • Note!!! The plot interpolates over the holes in the curve by displaying the value from the right data point. • SAS macro ICE from IML: NPMLE with CIs. 4 options for ML algorithms (Turnbulls self-consistency algorithm, Newton-Raphson Ridge, Quasi-Newton, Conjugate gradient). • The produced plots have holes in the curve for all intervals. Hypothesis testing: • Must program explicitly
300 mg Infusion Infusions Response Evaluation Follow-up Contact Example: Effect of Ofatumumab in patients with Follicular Lymphoma Treatment Follow-up Extended Follow-up Period Period Period 8 infusions 1000 mg N=86 Randomization 500 mg N=31 Scr 0 8 3 6 9 12 18 24 3 4 5 Weeks Months Years Visits
Conventionalsurvivalanalysisbasedon FDA approach Estimated percentage alive and not progressed
Interval censoring approach withTurnbullestimator and generalizedlog-rank test Estimated percentage alive and not progressed
Comparison Estimated percentage alive and not progressed
Progressed or Dead Entry * Patients dying without observed progr. have been assumed to have died without progressive disease:
Entry (Stage 1) Progressed (Stage 2) Dead (Stage 3) The real situation with PFS
Mortality introduces 2 problems • May miss progressions ifsubjects die beforebeingbetweenexaminations (interval censoring) • Biased (upwards) estimation of TTP • Can’tdefine marginal distribution of time to progression • Meaningless to considerrisk of progression afterdeath • Use (integrated) hazardsinstead of probabilities
Frydman & Szarek approach • Non-parameteric Markov model • Integrals simplify to finite sums • Hazard contributions to progressions and deaths on non-overlapping sets • Death: at the observed death times • Progression: on intervals between the death times • For progression hazard, the mass is concentrated on (P,Q] intervals generated from L,R,T
Contribution to likelihood from subjectwithobserved progression: Entry (Stage 1) Progressed (Stage 2) Dead (Stage 3) Frydman & Szarek approach Stay in (2) from Qj to T Die or censor at tr=T Don’t exit (1) before (Pj,Qj] Make (1)-(2) transition In (Pj,Qj] Similarexpression for subjectswhere progression is not observed but with an additional term for dyingdirectly from state 1
Example: PFS for Cetuximab+RT • C+RT vs RT • PD assessed @ w4, w8, + every 4 months for 2 years, then every ½ year during year 3-5 • Endpoint: PFS • PD assigned to first time where PD observed • If no PD observed prior to death assume death occurred directly from state 1 • If censored at end of follow-up, censor at time of last PD assessment • In accordance with FDA guidance
Example: PFS for Cetuximab+RT • N=424 randomized • 207 had observed PD (of which 78.3% died prior to study end) • 214 had noobserved PD prior to deathorstudy end • 53 wasassumed to have dieddirectly from stage 1 • 163 was right censored at last tumor assessment • 3 wereknown not to have PD and werealive at study end
Fouranalysismethods • Analysis I. Original analysis (the FDA method) Observed PD times analyzed as interval censored: • Analysis II: No other changes • Analysis III: Naive scenario (pts without observed PD or death are right censored for PFS at censoring time for death rather than at the last tumor ass.). • Analysis IV: New method accounting for the observations with missing status of the intermediate transition.
Results • Accounting for interval censoring decreases the estimated median PFS time for the RT group • The largest difference in 2-year PFS proportion is seen in Analysis IV
Estimated proportion with event F12 F=F12+F13 F13
Summary of challengesfoundwith interval censoringmethods • Convergence • If failure time is a mixture of interval censored observations and exact events. • How to plot the estimatedsurvivalfunction • If event studied is a compositeendpointlike PFS • Hypothesistesting • To whatextendwillanalysisresultsbeaccepted by authorities