Download
1 / 1
10 likes | 202 Views
EGDG 2010 ANNUAL MEETING “COMPREHENSIVE MANAGEMENT OF DYSPHAGIA” THESSALONIKI, 24-26 SEPTEMBER 2010. DIAGNOSIS AND MANAGEMENT OF ASPIRATION POST HEMILARYNGECTOMY Stefanidis A 1 , Kynigou M 1 , Aggeli D 1 , Soldatou S 1 , Eleytherakis A 1 , Triaridis A 1 ,

E N D
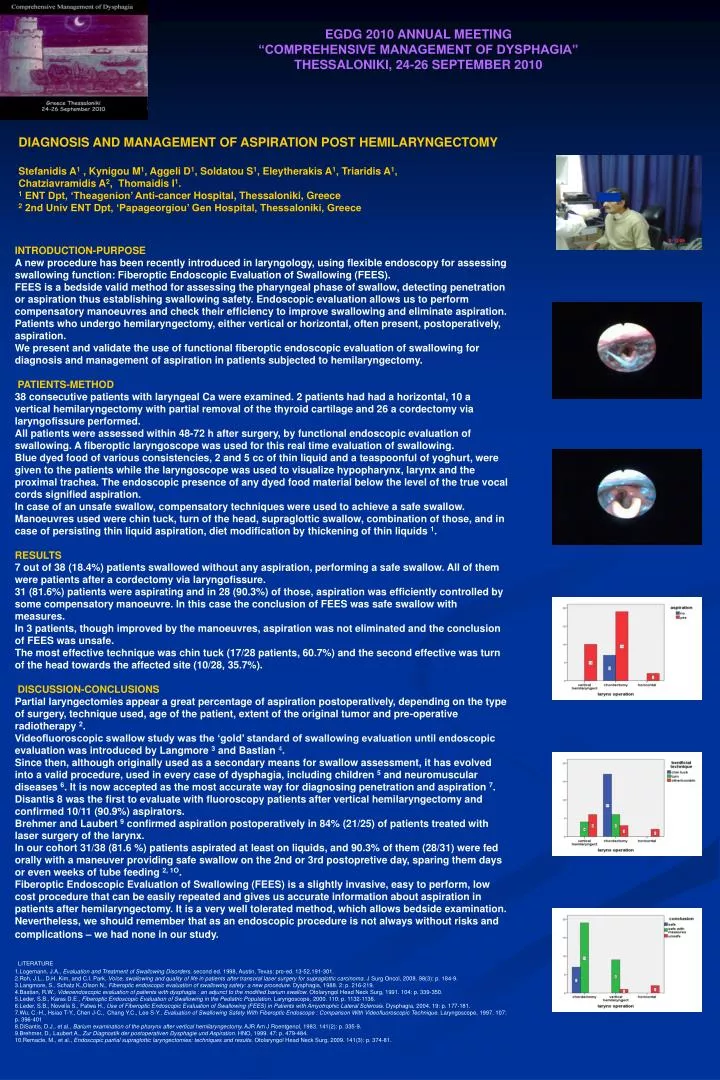
EGDG 2010 ANNUAL MEETING “COMPREHENSIVE MANAGEMENT OF DYSPHAGIA” THESSALONIKI, 24-26 SEPTEMBER 2010 DIAGNOSIS AND MANAGEMENT OF ASPIRATION POST HEMILARYNGECTOMY Stefanidis A1 , Kynigou M1, Aggeli D1, Soldatou S1, Eleytherakis A1, Triaridis A1, Chatziavramidis A2, Thomaidis I1. 1ENT Dpt, ‘Theagenion’ Anti-cancer Hospital, Thessaloniki, Greece 2 2nd Univ ENT Dpt, ‘Papageorgiou’ Gen Hospital, Thessaloniki, Greece INTRODUCTION-PURPOSE A new procedure has been recently introduced in laryngology, using flexible endoscopy for assessing swallowing function: Fiberoptic Endoscopic Evaluation of Swallowing (FEES). FEES is a bedside valid method for assessing the pharyngeal phase of swallow, detecting penetration or aspiration thus establishing swallowing safety. Endoscopic evaluation allows us to perform compensatory manoeuvres and check their efficiency to improve swallowing and eliminate aspiration. Patients who undergo hemilaryngectomy, either vertical or horizontal, often present, postoperatively, aspiration. We present and validate the use of functional fiberoptic endoscopic evaluation of swallowing for diagnosis and management of aspiration in patients subjected to hemilaryngectomy. PATIENTS-METHOD 38 consecutive patients with laryngeal Ca were examined. 2 patients had had a horizontal, 10 a vertical hemilaryngectomy with partial removal of the thyroid cartilage and 26 a cordectomy via laryngofissure performed. All patients were assessed within 48-72 h after surgery, by functional endoscopic evaluation of swallowing. A fiberoptic laryngoscope was used for this real time evaluation of swallowing. Blue dyed food of various consistencies, 2 and 5 cc of thin liquid and a teaspoonful of yoghurt, were given to the patients while the laryngoscope was used to visualize hypopharynx, larynx and the proximal trachea. The endoscopic presence of any dyed food material below the level of the true vocal cords signified aspiration. In case of an unsafe swallow, compensatory techniques were used to achieve a safe swallow. Manoeuvres used were chin tuck, turn of the head, supraglottic swallow, combination of those, and in case of persisting thin liquid aspiration, diet modification by thickening of thin liquids 1. RESULTS 7 out of 38 (18.4%) patients swallowed without any aspiration, performing a safe swallow. All of them were patients after a cordectomy via laryngofissure. 31 (81.6%) patients were aspirating and in 28 (90.3%) of those, aspiration was efficiently controlled by some compensatory manoeuvre. In this case the conclusion of FEES was safe swallow with measures. In 3 patients, though improved by the manoeuvres, aspiration was not eliminated and the conclusion of FEES was unsafe. The most effective technique was chin tuck (17/28 patients, 60.7%) and the second effective was turn of the head towards the affected site (10/28, 35.7%). DISCUSSION-CONCLUSIONS Partial laryngectomies appear a great percentage of aspiration postoperatively, depending on the type of surgery, technique used, age of the patient, extent of the original tumor and pre-operative radiotherapy 2. Videofluoroscopic swallow study was the ‘gold’ standard of swallowing evaluation until endoscopic evaluation was introduced by Langmore 3 and Bastian 4. Since then, although originally used as a secondary means for swallow assessment, it has evolved into a valid procedure, used in every case of dysphagia, including children 5 and neuromuscular diseases 6. It is now accepted as the most accurate way for diagnosing penetration and aspiration 7. Disantis 8 was the first to evaluate with fluoroscopy patients after vertical hemilaryngectomy and confirmed 10/11 (90.9%) aspirators. Brehmer and Laubert 9 confirmed aspiration postoperatively in 84% (21/25) of patients treated with laser surgery of the larynx. In our cohort 31/38 (81.6 %) patients aspirated at least on liquids, and 90.3% of them (28/31) were fed orally with a maneuver providing safe swallow on the 2nd or 3rd postopretive day, sparing them days or even weeks of tube feeding 2, 1O. Fiberoptic Endoscopic Evaluation of Swallowing (FEES) is a slightly invasive, easy to perform, low cost procedure that can be easily repeated and gives us accurate information about aspiration in patients after hemilaryngectomy. It is a very well tolerated method, which allows bedside examination. Nevertheless, we should remember that as an endoscopic procedure is not always without risks and complications – we had none in our study. LITERATURE 1.Logemann, J.A., Evaluation and Treatment of Swallowing Disorders. second ed. 1998, Austin, Texas: pro-ed. 13-52,191-301. 2.Roh, J.L., D.H. Kim, and C.I. Park, Voice, swallowing and quality of life in patients after transoral laser surgery for supraglottic carcinoma. J Surg Oncol, 2008. 98(3): p. 184-9. 3.Langmore, S., Schatz K.,Olson N., Fiberoptic endoscopic evaluation of swallowing safety: a new procedure. Dysphagia, 1988. 2: p. 216-219. 4.Bastian, R.W., Videoendoscopic evaluation of patients with dysphagia : an adjunct to the modified barium swallow. Otolaryngol Head Neck Surg, 1991. 104: p. 339-350. 5.Leder, S.B., Karas D.E., Fiberoptic Endoscopic Evaluation of Swallowing in the Pediatric Population. Laryngoscope, 2000. 110: p. 1132-1136. 6.Leder, S.B., Novella S., Patwa H., Use of Fiberoptic Endoscopic Evaluation of Swallowing (FEES) in Patients with Amyotrophic Lateral Sclerosis. Dysphagia, 2004. 19: p. 177-181. 7.Wu, C.-H., Hsiao T-Y., Chen J-C., Chang Y.C., Lee S-Y., Evaluation of Swallowing Safety With Fiberoptic Endoscope : Comparison With Videofluoroscopic Technique. Laryngoscope, 1997. 107: p. 396-401 8.DiSantis, D.J., et al., Barium examination of the pharynx after vertical hemilaryngectomy. AJR Am J Roentgenol, 1983. 141(2): p. 335-9. 9.Brehmer, D., Laubert A., Zur Diagnostik der postoperativen Dysphagie und Aspiration. HNO, 1999. 47: p. 479-484. 10.Remacle, M., et al., Endoscopic partial supraglottic laryngectomies: techniques and results. Otolaryngol Head Neck Surg, 2009. 141(3): p. 374-81.