Download

1 / 11
110 likes | 358 Views
Two Cases of Subconjunctival Bevacizumab Injection to Prevent Bleb Failure after Trabeculectomy. Dongwook Lee, Min Ahn, In-Cheon You, Daegyu Lee Chonbuk National University Medical School, Korea Authors have no financial interests in this presentation. Purpose.

E N D
Two Cases of Subconjunctival Bevacizumab Injection to Prevent Bleb Failure after Trabeculectomy Dongwook Lee, Min Ahn, In-Cheon You, Daegyu Lee Chonbuk National University Medical School, Korea Authors have no financial interests in this presentation
Purpose • Angiogenesis plays a important role in wound healing process, but it is an unwanted process after trabeculectomy. • Bleb failure involves vascularization with fibroblast migration and scarring of the fistula tract. • Vascular Endothelial Growth Factor (VEGF) is a unique mitogen specific to vascular endothelial cells and the signal cascade leading to fibroblast migration and proliferation involves dynamic interaction between many cytokines.
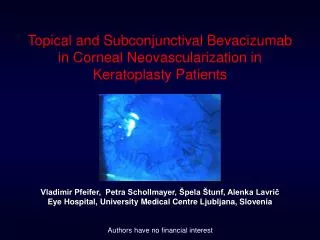
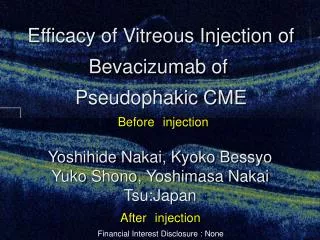
Purpose • Blocking the neovascular signal cascade with anti-VEGF molecules like Bevacizumab may lead to a decrease in fibroblast proliferation by decreasing the supply of mitogenic cytokines such as fibroblast growth factor (FGF) carried in by new vessel formation • We analyze the safety and efficacy of Subconjunctival Injection of bevacizumab (Avastin) for preventing bleb failure following trabeculectomy
Method • The clinical interventional case study included 2 patients with inflammatory glaucoma (Posner-Schlossman syndrome and Bechet’s disease) • Limbal based standard trabeculectomy was performed without mitomycin-C treatment. • Subconjunctival bevacizumab injections (1.25 ㎎/0.05 ㎖) was given at the end of the surgery adjacent to the bleb raised using a single-use 26 gauge needle and syringe.
Method • Patients characteristics
Results • Case 1 • A 37 years old male with Posner-Schlossman syndrome on his right eye • Uncontrolled intraocular pressure (around 40mmHg) with the maximum glaucoma medications and steroid (40 mg/day) administration. • Visual field defect (MD, -14dB) and disc cupping • Trabeculectomy with Subconjunctival bevacizumab injections • Post operative 2nd week, additional bevacizumab (1.25 mg/0.05 ㎖) injection under a slit lamp because of intense uveitis and increase vascular congestion and vascularization
Results • Case 2 • a 28 year old male suffering from Bechet’s disease and uveitis in both eyes • about 50% peripheral anterior synechiae of iris through a gonioscopy, and glaucoma-induced changes in optic discs which had a decreased sensitivity of -10 dB in the visual field test • Trabeculectomy with Subconjunctival bevacizumab injections
Case 1 patient (1a) Single layer of limbus- based flap and subconjunctival Bevacizumab injection. (1b) Post-operation 1 month photography. Note conjunctival injection and ketatic precipitates on lower half cornea due to iridocyclitis but bleb area shows no vascularization.
Case 2 patient (2a) Post-operation 1 day photography. (2b) 3 months after trabeculectomy with subconjunctival Bevacizumab injection. Note the well functioning bleb.
Intraocular pressure(IOP) changes following trabeculectomy with subconjunctival Bevacizumab injection.
Conclusion • The clinical interventional study included 2 patients with secondary glaucoma associated with uveitis • Subconjunctival bevacizumab to prevent bleb failure after trabeculectomy show good results • No adverse incidents were observed