Download
1 / 20
200 likes | 352 Views
Plan of the Day. Why bother ProceduresComplicationsRecommendationsEBM ProblemsScenario Revisited. Why Bother?. Patient has already had surgery

E N D
1. Aftercare Following Weight Loss Surgery Gray N. Dawson, MD, FAAFP
Lieutenant Commander, Medical Corps, U.S. Navy
Officer in Charge / Senior Medical Officer
U.S. Navy Branch Health Clinic St. Mawgan UK
2. Plan of the Day Why bother
Procedures
Complications
Recommendations
EBM Problems
Scenario Revisited
3. Why Bother? Patient has already had surgery � not addressing recommendations for or against bariatric surgery
Scenario:
Busy family medicine clinic
49 y/o female pt on schedule for �F/u labs�
CC: �I just moved to the area and need my six-month f/u appt following gastric bypass�
Questions:
What labs do I need to order?
What complications should I be looking for?
What is a realistic goal for the patient?
4. What you likely already know about Bariatric Surgery: Better weight loss than diet and exercise
Decrease disease burden
DM, HTN, lipids, CAD, arthritis, sleep apnea, fatty liver, metabolic syndrome, GERD & PCOS
Generally safe, but with many complications and consequences (change lifestyle)
Recommended for (by NIH consensus 1991):
Refractory obesity (BMI >35) with disease burden
Morbid obesity (BMI >40)
Covered by Tricare
� To be covered, you must be 100 pounds over ideal body weight and have a co-morbidity or 200 percent of ideal body weight with no co-morbidity� https://www.triwest.com/triwest/default.html?/triwest/unauth/content/provider/handbook/provider/imp_tricare_policy.html
5. What you may not know about bariatric surgery: Elderly � covered by Medicare, little study on this age population
Pediatrics � 1000 cases done in 2003 and increasing
Risks are highly variable depending greatly on experience / skill of surgeon
Death rate: approx 1.5-1.9%
Complications: up to 70% in studies
6. Procedures Three types of procedures:
Malabsorptive (reduce calorie absorption)
Biliopancreatic diversion (+/- duodenal switch)
Restrictive (reduce volume)
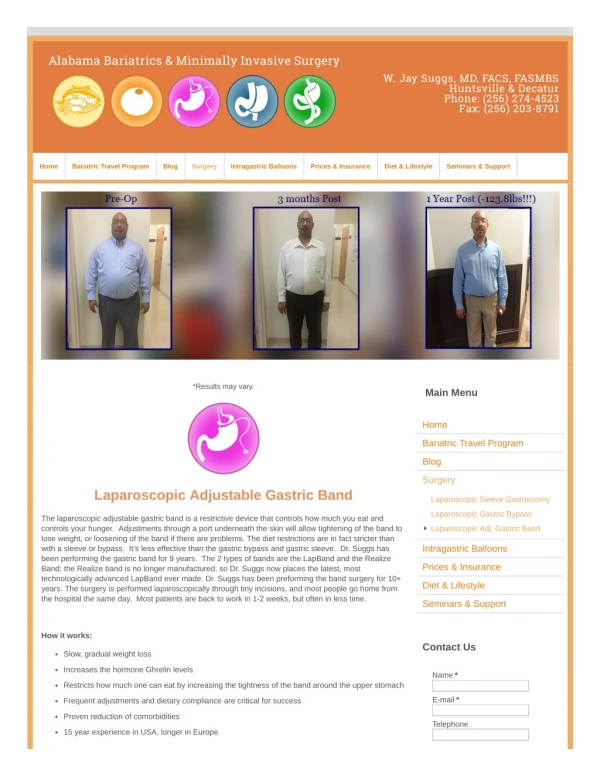
Vertical gastric banding
Laparoscopic adjustable gastric banding
Gastric bypass (both)
Roux-en-Y (laparoscopic / open)
Choice of procedure depends on patient, health status, & surgeon (experience)
Malabsorptive procedure (BPD) recommended for severe morbid obesity (BMI >50)
7. Short term complications Venous thromboembolism
Wound infection (greater with open procedures)
GI leaks (greater with laparoscopic and low experience)
Bleeding
Incisional hernia
Stomal stenosis (vomiting / intolerance to food and fluids)
Marginal ulceration (hematemesis / melena � avoid NSAIDs)
Constipation (pain meds, poor fluids, malabsorption; avoid granular bulking agents)
8. Complications: Vomiting Early: related to dietary factors such as poor chewing or too much intake
Mid (3-6 months): same, also consider thiamine deficiency
Late (>6 months): same, plus consider stomal stenosis
9. Complications: Dumping Syndrome Related to intake of high sugar foods/fluids
Undigested CHO causes rapid fluid influx in jejunum causing procholinergic symptoms:
Diarrhea / crampy abdominal pain
Nausea
Lightheadedness
Palpatations / sweating
Generally avoidable with dietary modification, not seen as much with complex natural sugars (fruits / vegetables)
10. Complications: Gallstones Frequent complication, generally GB removed at time of bariatric surgery if gallstones present prior to surgery surgery
If not removed, ursodeoxycholic acid prescribed up to six months � poor evidence for use
Surgery is best treatment if symptoms develop
Tricare and many other insurers do not cover removing prophylactically without symptoms
11. Complications: Drug Absorption Change in gastric pH
Change in volume of distribution with weight loss
Change in intestinal surface area
Need to monitor effects from medications, especially thyroid, psychiatric, epilepsy, DM, and HTN meds
12. Complications: Nutritional Deficiency Most commonly associated with malabsorptive procedures and include the following:
Iron
Calcium
Vitamin D
Vitamin B12
Fat Soluble Vitamins
Protein
Thiamine
Folate
13. Nutritional Recommendations MVI or PNV with Iron
May need additional supplemental iron up to 40-60mg/day elemental
B12 (100-300mcg/day � higher if deficient)
May need monthly 1mg injections
Calcium w/ Vit D (1200mg/day; 400IU/day)
Recommended calcium citrate vs. carbonate since low pH is required for CaCO3
Some suggest up to 1500mg/day calcium and 1000IU Vitamin D to prevent bone mineral density loss
High protein diet (lean protein)
14. Screening Recommendations First Year:
q3 months: CBC, Glu, Cr
q6 months: LFT (w/ protein, albumin), Ferritin, TIBC, B12, Folate, Ca
[PTH] (if Ca elevated or to ensure Ca stable)
[Vit D] (possibly to ensure adequate Ca)
Every year thereafter:
All of the above
Postmenopausal women: BMD Screening
Variable recommendations, probably worth screening and ensuring maximum calcium / vit D tx if low BMD
15. Family Planning Recommendations No pregnancy for female patients for 18 months
Contraception needs may change with weight loss
Pregnancy even later can be problematic and may need more frequent screening or more aggressive preventive treatments
B12, Folate, Iron
16. Show me the evidence� Retrospective / case series / cohort
Very few good RCTs
Does it improve long-term survival?
Flum (2004): Mortality at 15 years, N=3,328
Operated: 11.8%
Non-operated: 16.3%
Does it improve long-term QOL?
Difficult to measure, no good studies
Still many good long term retrospective / cohort studies 2800 studies reviewed by Cochrane, 18 selected for inclusion� denoted: need greater amount of good RCTs.2800 studies reviewed by Cochrane, 18 selected for inclusion� denoted: need greater amount of good RCTs.
17. Evidence Bariatric surgery leads to sustainable weight loss and may reduce weight related co-morbidities (SOR=A)
Prophylaxis to prevent VTE (DVT / PE) postoperatively using LMW heparin is indicated in nearly all patients (SOR=A)
Other recommendations based on incidence of disease and/or expert opinion such as pregnancy recommendations, screening recommendations, and nutritional supplementation (SOR=B/C)
See www.aafp.org/afpsort.xml for more info on SORT
18. Scenario Revisited What do I need to order:
CBC, iron studies, LFT (albumin / protein), Ca, Glu, Cr, B12, Folate (expert opinion)
Some suggest PTH/VitD, BMD scan yearly
PNV, Ca w/ Vit D, Iron, B12, Folate
What complications should I be looking for:
No longer menstruating (no contraceptives)
Nutritional deficiencies, esp. iron, B12, protein, calcium
Gallstone dz or post-surgery complications
Psychologic impacts of lifestyle changes
What is a realistic goal:
Weight loss of approximately 35-70% of excess or sustained 45-65 lbs at 10 years (avg.)
19. For More Information Viriji A, Murr MM. Care for Patients After Bariatric Surgery. Am Fam Phys 2006;73:1403-8.
http://www.aafp.org/afp/20060415/1403.html
Good general overview
Stendardo, S, Kushner PR. Caring for Patients After Bariatric Surgery. CME Bulletin (AAFP) 2006;5(2):1-6.
http://www.aafp.org/online/etc/medialib/aafp_org/documents/cme/selfstudy/bulletins/bariatricbulletin.Par.0001.File.dat/cmebulletin_bariatric.pdf
Good general overview
Mason ME, Jalagani H, Vinik AI. Metabolic Complications of Bariatric Surgery: Diagnostic and Management Issues. Gastroenterol Clin N Amer 2005;34:25-33.
Review of metabolic problems for follow-up
F. Safadi, Trends in Insurance Coverage and Impact of Evidence Based Reviews, Surg Clin N Amer 2005;85:665-680.
Great EBM Review
Brechner RJ, Farris C, Harrison S, Tillman K, Salive M, Phurrough S. Summary of Evidence � Bariatric Surgery, Center for Medicare Studies, November 4, 2004, retrieved from:
http://www.cms.hhs.gov/FACA/downloads/id137c.pdf
Great EBM Review
20. Further Bibliography� Ali MR, Fuller WD, Choi MP, Wolfe BM. Bariatric Surgical Outcomes. Surg Clin N Am 2005;85:835-852.
Li Z, Bowerman S, Heber D. Health Ramifications of the Obesity Epidemic. Surg Clin N Am 2005;85:681-701.
Livingston EH. Complications of Bariatric Surgery. Surg Clin N Am 2005;85:853-868.
Neligan PJ, Williams N. Nonsurgical and Surgical Treatment of Obesity. Anesthesiology Clin N Amer 2005;23:501-523.
Puzziferri N. Psychologic Issues in Bariatric Surgery � the Surgeon�s Perspective. Surg Clin N Am 2005;85:741-755.
Stumbo P, Hemingway D, Haynes WG. Dietary and Medical Therapy of Obesity. Surg Clin N Am 2005;85:703-724.
Xanthakos SA, Daniels SR, Inge TH. Bariatric Surgery in Adolescents: An Update. Adolesc Med 2006;17:589-612.