Download

1 / 51
520 likes | 1.19k Views
BUDGETING FOR NURSING SERVICE. Start your day with hope, but end it with accomplishment.

E N D
Start your day with hope, but end it with accomplishment.
Healthcare organizations are increasingly focused on cost-containment and efficacious use of financial resources. Today’s nursing leaders require budgeting knowledge in order to efficiently manage operations in the patient care environment and meet financial targets.
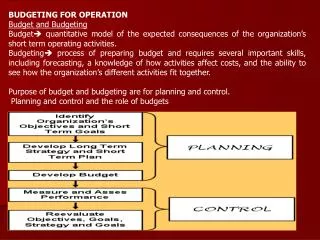
Budgets A budget is a detailed financial plan, used to carry out organizational goals. The budget includes proposed earnings and expenditures as well as details about how resources( money, time, and people) will be acquired and used. The purpose of the budget is to project future plans and costs.
Operating budget-deals primarily with salaries, supplies, and contractual services It is the financial plan for the day to day activities of the organization containing a statement of expected revenues and expenses for the fiscal year. Revenue Budget- includes expected income based on volume and mix of patients, rates, and discounts. Expense Budget- includes salary and non-salary items that reflect patient care objectives and planned activities for the nursing unit.
Cost and Profit Cost Center-the smallest area for which costs are accumulated. They may produce revenue, such as laboratory and radiology or not produce revenue, such as nursing. Profit Center- a unit where performance is measured in terms of profit the difference between revenues and expenses
Classification of Costs Fixed Costs-expenses that remain the same such as rent or insurance premiums. Variable costs-expenses that change with changes in volume and acuity. Mixed Costs-may vary with volume but not directly. Direct Costs-affect patient care.
Salary (Personnel) Budget The personnel budget projects the salary costs that will be paid and charged to the cost center. It accounts for replacement of staff for benefit time, overtime, shift differentials, orientation, on-call hours, bonuses and premiums, and salary increases.
Variance Analysis The difference between the amount that was budgeted for a specific revenue or cost and the actual revenue or cost that resulted during the course of activities is known as the variance. There is an established level at which a variance needs to be investigated. A variance may be favorable or unfavorable and may be related to patient volume, efficiency in relation to nursing care hours provided, rates in hourly rates paid, or in non-salary expenditures Position Control- a tool to monitor actual numbers of employees to the number of FTE’s budgeted.
Why you need budgeting skills • Absolutely essential management skill • Financial viability • Quality patient care • Unit operational efficiency • Staff satisfaction • Leadership expectation • Most nurse managers do not come into • the job with these skills
Capital Budgeting Process
Identify immediate needs • New services • New technology • Broken equipment
Identify Long-term needs • New services • New patient populations • New technology • Improved technology • Equipment replacement plan • Elimination of rentals
Give what they want Get input MDs (Intensivists, surgeons, cardiologist,specialists) RN Staff Respiratory Therapy Ancillary staff
Vendors Develop (compliant) vendor relationships throughout the year Be aware of contracted vendors Become knowledgeable about products Ask for demos Ask for references (and check them) Evaluate the literature provided to you Drive a hard bargain Don’t forget trade-in value Consider contract for training costs
Hidden Sources • Investigate sources of funding • Technology committees • Specialty funds • Workplace safety funds • Patient safety funds • Equipment used in Clinical Trials • Vendor trials • Contingency Funds
Make a convincing case • How does this equipment improve • quality of patient care? • Is it a regulatory compliance issue? • Will it improve patient safety? • Will it improve staff safety? • Will it save you money in the long • run?
Final Advice • Be mindful of deadlines • Allow enough time for each step of the • process • Vendor response time • Paperwork • Local/regional/corporate approvals • Fiscal year
Budget Variance in the Operating Budget WHY ARE YOU OVER BUDGET?
Budget Variance • Payroll budget • Non-payroll budget
Non-payroll Operating Budget • Supply Costs • Equipment Costs • Operational Costs
Non-payroll costs • Unit upkeep / construction • Operational Costs • Education • Conference fees • References materials • Employee recognition
Non-payroll (cont.) • Transportation • Traveler housing • One-time expenses • Lost patient belongings
Supply Costs Ask yourself, “Is there a change in the supply OR a change in the patients?”
Change in supply cost • New product • Change in cost of product • Change in vendor • Change in contract price • Substitute product • Stocking Issues
Change in Patient • Change in volume • Change in patient population • Individual patient need
Equipment Cost • Purchases • Rentals • Maintenance • Vendor change • Contract Change • Consider capitated costs for rentals
Payroll Budget Simply put… What you pay the people who take care of the patients
Payroll Budgeting Tips Budget to full-time equivalents (FTEs) and dollars Account for inflation and salary increases Factor in contractual obligations Estimate non-productive time Account for anticipated changes in patient volume and acuity
Payroll budget Volume Acuity Overtime Pay Penalty Pay Registry and Traveler Pay Payroll Variance Volume HPPD CPPD
Volume January Patient Days Budgeted = 310 Actual = 434 Variance = 124 To calculate volume variance: Variance days/budgeted days 124/310 = .4 Conclusion: You are 40% over your budgeted volume!
Summary of Variance • Examine Payroll and Non-payroll costs • Look at both in relation to volume • Non-payroll • Supply cost • Equipment costs • Other operating costs Payroll • Payroll • OT and Registry Usage • Training Costs • Concisely explain why
Developing a Staffing Matrix Required information Predicted/budgeted average daily census (ADC) Historical trends Population changes/changes in case mix Changes in service/specialty offerings
Hours Per Patient Day HPPD = number of hours worked in the 24 hour period divided by the midnight census Example NOC shift staffed with 4 RNs DAY shift staffed with 5 RNs and a NA PM shift staffed with 5 RNs and a NA Midnight census = 8 HPPD = (16 employees x 8 hours) / census of 8 = 128/8=16
Cost Per Patient Day CPPD = [(Total RNs * 8 hours) * hourly salary + (Total LVNs * 8 hours) * hourly salary + (Total NAs * 8 hours) * hourly salary)] /divided by midnight census
Developing a Position Control Document Required information Budgeted Average Daily Census (ADC) Required full-time equivalents (FTEs) in each job category (from staffing matrix) Current hired FTEs in each job category per shift Current Posted FTEs in each job category per shift Historical use of non-productive time
ANALYSIS 1. What can we determine from this position control document? 2. Have we budgeted for enough staff? 3. Do we currently have enough staff? 4. What additional positions would we need to post?
Step one: Review past performance: 1. As a starting point, the nurse executive will require to review the following
a. The financial records from prior financial periods as a basis for planning. b. The present activities of the nursing division.
c. The activities that the division plans to institute during the projected financial period. d. Those activities the division plans to delete during the projected period.
Step two: Review the organization's goals and projections: • The nurse executive has to study the organization's goals and financial projections thoroughly. - Items in the major budgetary report that affect the nursing department should be determined
Step three: Review of the variances with higher levels of management : • Once the goal statement is finished, it, (together with the actual versus budget analysis done earlier), should be reviewed with higher level management
The departmental goals proposed should be carefully considered; as well as the variances, their causes, and proposed corrective actions should be reviewed. • Once the final statement for the department is in place, the new budgeting process can begin in earnest.
Step four: Actual preparation of the budget: • The actual preparation of a new budget can be done based on a previous budgetary plan, or newly proposed plan (if a newly developed or modified service).
To complete the budget, a budget worksheet is essential. Worksheet is "a tool used by managers to prepare their budget". It includes a number of columns including information about:
a) Historic information with old budget. b) Actual numbers with comments explaining the variances. c) Revenue and costs.
What have you learned? • Capital Budget • Identify short and long-term needs • Work effectively with vendors • Plan ahead and allow lots of time • Analysis of Operating Budget variance • Payroll • Non-payroll • Staffing Matrices • Position Control
The quickest way to get what you want is to help others get what they want.
SHIFT TO POPULATION BASED CARE AND INCREASING COMPLEXICITY OF PATIENT CARE