Download
1 / 20
220 likes | 582 Views
RENAAL Altering the Course of Renal Disease in Hypertensive Patients with Type 2 Diabetes and Nephropathy with the A II Antagonist Losartan. RENAAL. R eduction of E ndpoints in N IDDM with the A II A ntagonist L osartan.

E N D
RENAAL Altering the Course of Renal Disease in Hypertensive Patients with Type 2 Diabetes and Nephropathy with the A II Antagonist Losartan
RENAAL Reduction of Endpoints in NIDDM with the AIIAntagonist Losartan An investigator initiated, multicenter, double-blind, randomized, placebo-controlled study to evaluate the renal protective effects of losartan in hypertensive patients with Type 2 diabetes and nephropathy 1513 Patients; 250 Centers; 28 Countries • Steering Committee Chair B. M. Brenner, MD • Data and Safety Monitoring Committee Chair C.E. Mogensen, MD • Clinical Endpoint Adjudication Committee Chair S. Haffner, MD • Coordinating Center: Merck Research Labs Study Director S. Shahinfar, MD Brenner BM et al New Engl J Med2001;345(12):861-869.
RENAAL Primary Hypothesis Long-term treatment with losartan versus placebo (alone or in combination with conventional anti hypertensive therapy*) in Type 2 diabetic patients with hypertension and nephropathy will increase the time to first event and decrease the incidence of doubling of sCr, ESRD or death. * Excluding ACEIs and other AIIAs Brenner BM et al New Engl J Med2001;345(12):861-869.
RENAAL Secondary Hypothesis • Losartan compared to placebo (alone or in combination with conventional antihypertensive therapy*) in hypertensive patients with Type 2 diabetes and nephropathy will: • increase the time to first event and decrease the incidence of cardiovascular morbidity/mortality • reduce proteinuria • decrease the rate of progression of renal disease * Excluding ACEIs and other AIIAs Brenner BM et al New Engl J Med2001;345(12):861-869.
RENAAL Study Design Losartan 100 mg qd (+CT) Losartan 100 mg qd (+CT) Losartan 50 mg qd (+CT) Maintain conventional antihypertensive therapy (CT)* (excluding ACEI, AIIA) Goal trough BP: < 140/<90 mmHg n=1513 Placebo (+CT) Placebo (+CT) Placebo (+CT) 6 Wks 4 Wks 8 Wks Mean follow-up 3.4 years *CT=conventional therapy: Open-label calcium-channel blocker, diuretic, beta blocker, alpha blocker, or centrally acting agents. Brenner BM et al J Renin-Angio-Aldo System 2000;1(4):328-335.
RENAAL Inclusion/Exclusion Criteria Inclusion criteria Type 2 diabetes Age 31-70 years Proteinuria:urine alb:cr >300 mg/g, >25 mg/mmol Serum Creatinine: 1.3-3.0 mg/dl, 115-265 µmol/L* Exclusion criteria Type 1 diabetes Known non-diabetic renal disease or renal artery stenosis Recent history of MI, CABG, PTCA, CVA, TIA History of heart failure HbA1c >12% *Lower limit 1.5 mg/dl (133 µmol/L) in male patients >60 kg Brenner BM et al J Renin-Angio-Aldo System 2000;1(4):328-335. Brenner BM et al New Engl J Med2001;345(12):861-869.
RENAAL Enrollment by Regionn=1513 Asia 17% North America 46% Europe 19% Latin America 18% Brenner BM et al New Engl J Med2001;345(12):861-869.
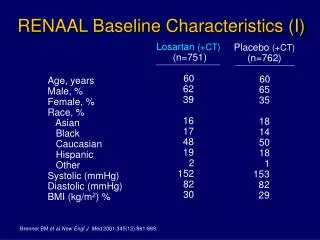
RENAAL Baseline Characteristics (I) Losartan (+CT) (n=751) 60 62 38 16 17 48 19 2 152 82 30 Placebo (+CT) (n=762) 60 65 35 18 14 50 18 1 153 82 29 Age, years Male, % Female, % Race, % Asian Black Caucasian Hispanic Other Systolic (mmHg) Diastolic (mmHg) BMI (kg/m2) % Brenner BM et al New Engl J Med2001;345(12):861-869.
RENAAL Primary Composite Endpoint and Components Losartan (+CT) (n=751) n (%) 327 (43.5) 162 (21.6) 147 (19.6) 158 (21.0) 255 (34.0) Placebo (+CT) (n=762) n (%) Composite and Components % Risk Reduction 16 25 28 -2 20 DsCr, ESRD, Death Doubling of sCr ESRD Death ESRD or Death P-Value 0.02 0.006 0.002 0.88 0.01 95% CI (2, 28) (8, 39) (11, 42) (-27, 19) (5, 32) 359 (47.1) 198 (26.0) 194 (25.5) 155 (20.3) 300 (39.4) Brenner BM et al New Engl J Med 2001;345(12):861-869.
30 20 10 30 0 0 12 24 36 48 P 20 L 10 50 0 40 0 12 24 36 48 30 20 10 0 0 12 24 36 48 RENAAL Primary Components ESRD Risk Reduction: 28% P p=0.002 % with event L Doubling of Serum Creatinine Risk Reduction: 25% p=0.006 Months P (+ CT) 762 715 610 347 42 L (+ CT) 751 714 625 375 69 % with event ESRD or Death Risk Reduction: 20% p=0.01 P % with event L Months P (+ CT) 295 762 689 554 36 L (+ CT) 52 751 692 583 329 Months P (+ CT) 762 715 610 347 42 L (+ CT) 751 714 625 375 69 Brenner BM et al New Engl J Med2001;345(12):861-869. 0902CZR01NL537SS0901
RENAALBlood Pressures (mmHg) Baseline Year 1 Year 2 Study End L (+CT) S/D 152/82 146/78 143/77 140/74 P (+CT) S/D 153/82 150/80 144/77 142/74 L (+CT) MAP 105.5 100.9 99.1 95.9 P (+CT) MAP 106.0 103.1 99.7 96.8 L (+CT) PP 69.4 67.8 66.2 66.7 P (+CT) PP 70.8 69.8 67.1 67.4 S/D: Systolic/Diastolic MAP: Mean arterial pressure PP: Pulse pressure L = losartan P = placebo CT = conventional therapy Brenner BM et al New Engl J Med 2001;345(12):861-869.
RENAALDose of Losartan • The daily dose of losartan ranged from 50-100 mg Losartan* n=751 % 71 100 mg QD *Patients who took the dose more than 50% of the time. Brenner BM et al New Engl J Med 2001;345(12):861-869.
RENAALConcurrent Antihypertensive Medications Losartann=751 77.9 60.7 83.8 40.2 34.1 18.0 Placebon=762 81.1 63.9 84.0 45.7 36.7 21.7 • Therapeutic Class • Calcium-Channel Blocker (%) • - Dihydropyridine (%) • Diuretic (%) • Alpha blocker (%) • Beta blocker (%) • Centrally acting agents (%) Brenner BM et al New Engl J Med 2001;345(12):861-869. .
RENAALSecondary Composite Endpointand Components Losartan (+CT)(N=751) n (%) 247 (32.9) 89 (11.9) 50 (6.7) Placebo (+CT) (N=762) n (%) 268 (35.2) 127 (16.7) 68 (8.9) Composite and Components % RiskReduction 10 32 28 P-Value 0.26 0.005 0.08 CV Morbidity/Mortality Heart Failure MI Brenner BM et al New Engl J Med 2001;345(12):861-869.
20 15 10 5 0 RENAALFirst Hospitalization for Heart Failure Risk Reduction: 32% p=0.005 P % with event L 0 12 24 36 48 Months P (+CT) 762 685 616 375 53 L (+CT) 751 701 637 388 74 L = losartan P = placebo CT = conventional therapy Brenner BM et al New Engl J Med 2001;345(12):861-869.
RENAALChange from Baseline in Proteinuria 40 20 P 0 Median Percent Change p<0.001 -20 35% Overall Reduction -40 L -60 0 12 24 36 48 Months P (+CT) 762 632 529 390 130 130 130 130 130 130 L (+CT) 751 661 558 438 167 167 167 167 167 167 Proteinuria measured as the urine albumin:creatinine ratio from a first morning void. L = losartan P = placebo CT = conventional therapy Brenner BM et al New Engl J Med 2001;345(12):861-869.
RENAALRate of Progression of Renal Disease (median 1/sCr Slope) p=0.01 18% reduction -.08 -0.069 -0.056 -.06 dl/mg/yr -.04 -.02 0 Losartan Placebo sCr=serum creatinine (+CT) (+CT) Brenner BM et al New Engl J Med 2001;345(12):861-869.
RENAAL Summary (I) • In hypertensive patients with Type 2 diabetes and nephropathy: • losartan delayed the onset of the primary composite endpoint (DsCr/ESRD/Death) and delayed the progression to ESRD. • losartan reduced proteinuria and the rate of decline in renal function (1/sCr slope). • losartan reduced the incidence of hospitalization for heart failure. • these benefits were largely independent of achieved blood pressure. Brenner BM et al New Engl J Med 2001;345(12):861-869.
RENAAL Summary (II) • In hypertensive patients with Type 2 diabetes and nephropathy: • losartan and placebo, on a background of conventional therapy, showed no significant difference on all-cause mortality, MI, stroke, revascularization, hospitalizations for unstable angina, and death due to CV disease. • losartan was generally well tolerated in this patient population. Brenner BM et al New Engl J Med 2001;345(12):861-869.
RENAALConclusions • Losartan confers significant benefits on renal outcomes in Type 2 diabetic patients with hypertension and nephropathy. • Losartan therapy results in a significant reduction in hospitalizations for heart failure. • Losartan is generally well tolerated. • Benefits of losartan seen in RENAAL complement many previous losartan studies which demonstrate a reduction in microalbuminuria and macroalbuminuria. Brenner BM et al New Engl J Med 2001;345(12):861-869.