Download
1 / 1
10 likes | 69 Views
Explore the effectiveness and safety of Stereotactic Body Radiotherapy (SBRT) in treating oligometastatic prostate cancer, aiming to defer Androgen Deprivation Therapy (ADT) and mitigate side effects. This study reviews outcomes of SBRT treatments in men with limited metastases and evaluates biochemical responses and ADT use. Results show potential for SBRT to control the disease and delay ADT requirement with manageable toxicity, suggesting a promising treatment option.

E N D
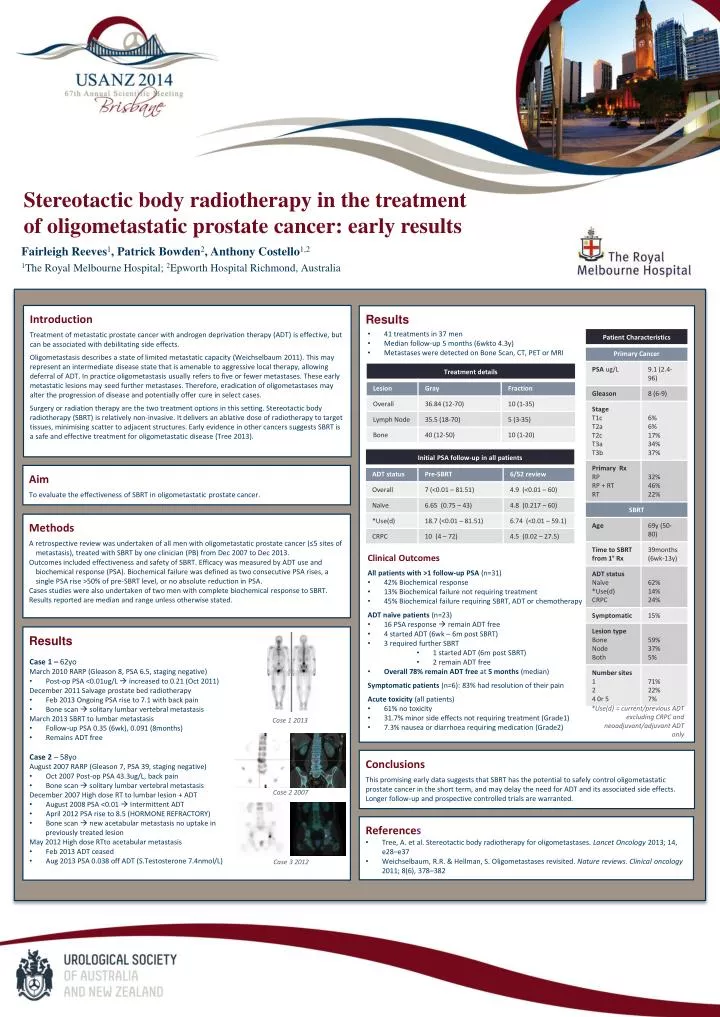
Stereotactic body radiotherapy in the treatment of oligometastatic prostate cancer: early results Fairleigh Reeves1, Patrick Bowden2, Anthony Costello1,2 1The Royal Melbourne Hospital; 2Epworth Hospital Richmond, Australia Introduction Treatment of metastatic prostate cancer with androgen deprivation therapy (ADT) is effective, but can be associated with debilitating side effects. Oligometastasis describes a state of limited metastatic capacity (Weichselbaum 2011). This may represent an intermediate disease state that is amenable to aggressive local therapy, allowing deferral of ADT. In practice oligometastasis usually refers to five or fewer metastases. These early metastatic lesions may seed further metastases. Therefore, eradication of oligometastases may alter the progression of disease and potentially offer cure in select cases. Surgery or radiation therapy are the two treatment options in this setting. Stereotactic body radiotherapy (SBRT) is relatively non-invasive. It delivers an ablative dose of radiotherapy to target tissues, minimising scatter to adjacent structures. Early evidence in other cancers suggests SBRT is a safe and effective treatment for oligometastatic disease (Tree 2013). Results • 41 treatments in 37 men • Median follow-up 5 months (6wkto 4.3y) • Metastases were detected on Bone Scan, CT, PET or MRI Aim To evaluate the effectiveness of SBRTin oligometastatic prostate cancer. Methods A retrospective review was undertaken of all men with oligometastatic prostate cancer (≤5 sites of metastasis), treated with SBRT by one clinician (PB) from Dec 2007 to Dec 2013. Outcomes included effectiveness and safety of SBRT. Efficacy was measured by ADT use and biochemical response (PSA). Biochemical failure was defined as two consecutive PSA rises, a single PSA rise >50% of pre-SBRT level, or no absolute reduction in PSA. Cases studies were also undertaken of two men with complete biochemical response to SBRT. Results reported are median and range unless otherwise stated. • Clinical Outcomes • All patients with >1 follow-up PSA (n=31) • 42% Biochemical response • 13% Biochemical failure not requiring treatment • 45% Biochemical failure requiring SBRT, ADT or chemotherapy • ADT naïve patients(n=23) • 16 PSA response remain ADT free • 4 started ADT (6wk – 6m post SBRT) • 3 required further SBRT • 1 started ADT (6mpost SBRT) • 2 remain ADT free • Overall 78% remain ADT free at 5 months (median) • Symptomatic patients (n=6): 83% had resolution of their pain • Acute toxicity (all patients) • 61% no toxicity • 31.7% minor side effects not requiring treatment (Grade1) • 7.3% nausea or diarrhoea requiring medication (Grade2) Results • Case 1 – 62yo • March 2010 RARP (Gleason 8, PSA 6.5, staging negative) • Post-op PSA <0.01ug/L increased to 0.21 (Oct 2011) • December 2011 Salvage prostate bed radiotherapy • Feb 2013 Ongoing PSA rise to 7.1 with back pain • Bone scan solitary lumbar vertebral metastasis • March 2013 SBRT to lumbar metastasis • Follow-up PSA 0.35 (6wk), 0.091 (8months) • Remains ADT free • Case 2 – 58yo • August 2007 RARP (Gleason 7, PSA 39, staging negative) • Oct 2007 Post-op PSA 43.3ug/L, back pain • Bone scan solitary lumbar vertebral metastasis • December 2007 High dose RT to lumbar lesion + ADT • August 2008 PSA <0.01 Intermittent ADT • April 2012 PSA rise to 8.5 (HORMONE REFRACTORY) • Bone scan new acetabular metastasis no uptake in • previously treated lesion • May 2012 High dose RTtoacetabular metastasis • Feb 2013 ADT ceased • Aug 2013 PSA 0.038 off ADT (S.Testosterone 7.4nmol/L) *Use(d) = current/previous ADT excluding CRPC and neoadjuvant/adjuvant ADT only Case 1 2013 Conclusions This promising early data suggests that SBRT has the potential to safely control oligometastatic prostate cancer in the short term, and may delay the need for ADT and its associated side effects. Longer follow-up and prospective controlled trials are warranted. Case 2 2007 • References • Tree, A. et al.Stereotactic body radiotherapy for oligometastases. Lancet Oncology2013; 14, e28–e37 • Weichselbaum, R.R. & Hellman, S. Oligometastases revisited. Nature reviews. Clinical oncology2011; 8(6), 378–382 Case 3 2012






