Download
1 / 68
680 likes | 818 Views
Launch of the report Dementia: ethical issues 1 October 2009. Introduction. Professor Albert Weale FBA Chair, Nuffield Council on Bioethics. The Nuffield Council on Bioethics. Established in 1991 Independent body that examines ethical questions raised by advances in biology and medicine

E N D
Launch of the report • Dementia: ethical issues • 1 October 2009
Introduction Professor Albert Weale FBA Chair, Nuffield Council on Bioethics
The Nuffield Council on Bioethics • Established in 1991 • Independent body that examines ethical questions raised by advances in biology and medicine • Contributes to policy making and stimulates debate
Dementia: ethical issuesThe report The report contains a number of conclusions and recommendations to policy makers in the following areas: • ethical approaches to dementia care • tackling dilemmas in day-to-day care • decision making • stigma and including people with dementia in society • recognising the needs of family carers • research priorities and participation
Launch of the report • Dementia: ethical issues • 1 October 2009
Dementia: ethical issues • Introduction and ethical framework • Professor Tony Hope • Chair of the Working Party on dementia and • Professor of Medical Ethics, University of Oxford
The Working Party • Began work in November 2007 • Members included those with expertise in medical ethics, front line care for people with dementia, law, old age psychiatry and neuroscience • Public consultation in July 2008 received over 200 responses • Deliberative workshop for 50 members of the public held in Birmingham
What is dementia? • Dementia is a disorder in which people experience a progressive decline in their mental ability because of damage to the brain • 700,000 people in the UK have dementia • This could rise to 1.7 million by 2051 • One in five people will develop dementia by the age of 85 • Dementia costs the UK more than £17 billion each year
An ethical framework for dementia • Six ‘components’ • A methodology for approaching ethical decisions • Two beliefs about the nature of dementia • A set of interlinked ethical values
An ethical framework: Component 1 • A ‘case-based’ approach to ethical decisions • Identify the relevant facts • Interpret and apply appropriate ethical values • Compare the situation with other similar situations
An ethical framework: Components 2 & 3 • Two beliefs about the nature of dementia • Dementia arises as a result of a brain disorder, and is harmful to the individual • With good care and support, people with dementia can expect to have a good quality of life – you can ‘live well’ with dementia
An ethical framework: Component 4 • Promoting the interests of the person with dementia and those who care for them 1. Promoting autonomy Autonomy is not just about ‘rational choice’ – it includes supporting important relationships, and supporting the person in expressing their values 2. Promoting well-being Well-being includes moment-to-moment experiences of contentment, and also objective factors such as a person’s level of mental ability
An ethical framework: Component 5 • Acting in accordance with solidarity • The belief that people with dementia are fellow citizens and that we are all ‘fellow-travellers’ • Recognition of our mutual interdependence • Duty to support people with dementia and to support carers in their own exercise of solidarity
An ethical framework: Component 6 • Recognising the personhood of the person • with dementia • A person with dementia is the ‘same’ person, despite changes in mood and behaviour • A person with dementia is of equal value to a person without dementia
Our view • Those who support and care for people with dementia need more support in tackling the ethical problems they meet every day • We conclude there is a need for: • Education – to help respond to dilemmas • Forums – to share and receive support
Launch of the report • Dementia: ethical issues • 1 October 2009
Dementia: ethical issues Ethical approaches to care Dr Rhona Knight FRCGP General Practitioner and member of the Nuffield Council on Bioethics
What is ethical care? Recognises the value of the person with dementia Aims to promote the well-being and autonomy of the person with dementia Pays attention to the interests of carers who provide day-to-day support
We conclude: 1.How things are done, will often be more important than the structure of services 2. Professionals and care workers should treat families as ‘partners in care’ What is ethical care?
Diagnosis Information, communication, signposting Ongoing care and support Acute hospital services End of life palliative care What is ethical care? 20
Diagnosis A timely diagnosis - for person and family Good quality assessment and support from initial concern Research needed on why some cultural groups appear hesitant in coming forward Encouragement to share information
Information, communication and signposting Need for Appropriate information Practical support Emotional support Access to services Dementia care advisor pilot
Ongoing care and support Flexibility to individual needs Importance of developing relationships with care workers Importance of care for the ‘small things’ Treating the person with dementia with dignity
Acute Hospital Services Often different needs Avoidance of unnecessary distress Examples of good practice
End of life palliative care Palliative, supportive and person centered care Less likely to receive good quality palliative Need for appropriate services Lots of development nationally We conclude We welcome the commitment in the English Dementia Strategy to develop and evaluate such models
Launch of the report • Dementia: ethical issues • 1 October 2009
Dementia: ethical issues • Dementia and society • Professor Ruud ter Meulen • Professor of Ethics in Medicine, • University of Bristol
Combating stigma • People with dementia may feel devalued and/or excluded from mainstream society • Our ethical framework emphasises the importance of equality for people with dementia • Information and awareness campaigns are only one part of the story – dementia must become an accepted, visible part of our society
Promoting inclusion • People with dementia need to feel comfortable carrying on with their usual activities, for example: • going to a club or out to lunch • participating in church activities • taking part in voluntary work • involvement in dancing, art and music
Promoting inclusion • Shops, restaurants and leisure facilities have a legal duty to enable people with dementia to use their services • However, they will often not realise this and even if they do, they are unlikely to have sufficient knowledge of dementia to make appropriate adjustments • We recommend • The Equality and Human Rights Commission should provide practical guidance on how to enable people with dementia to access services
Role of society in providing care • Many services required by people with dementia are classed as ‘social’ services • Funding arrangements in social care often mean that only ‘crisis’ cases receive appropriate care
Role of society in providing care • Component 2 of the ethical framework: “Dementia arises as a result of a brain disorder, and is harmful to the individual” • People with dementia should therefore have access to the care they need on the same basis as people with conditions such as cancer We conclude The availability of services needed by people with dementia should not be determined by classifications of care
Launch of the report • Dementia: ethical issues • 1 October 2009
Dementia: ethical issues • Research priorities • Professor Hugh Perry FMedSci • Professor of Experimental Neuropathy, University of Southampton and member of the Nuffield Council on Bioethics
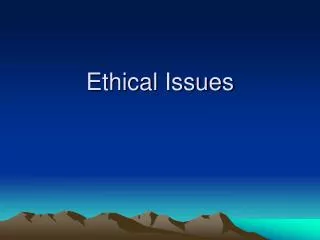
Combined research funding 2007-08 £ (million) Source: House of Commons Hansard 16/12/08
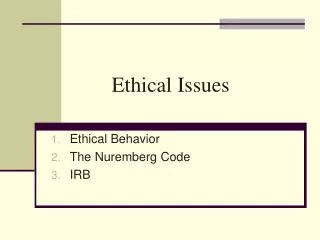
Research papers published since 2002 % of research papers Source: Knapp M and Prince M (2007) Dementia UK (London: Alzheimer’s Society), pxv.
Funding • We conclude • Major funders should explain more clearly how and why they divide their research funds between areas of research • More support and encouragement is needed for researchers who carry out high-quality research in dementia
Funding allocation within dementia research • We encourage more research into: • The experience of living with dementia • How people with dementia can be supported to live the best possible lives
Launch of the report • Dementia: ethical issues • 1 October 2009
Dementia: ethical issues • Making decisions • Professor Jill Peay • Professor of Law, • London School of Economics
What is the law? • People have the legal right to make their own decisions about health care and general welfare • As dementia progresses, it can get harder for people to make their own decisions • Decisions for people who lack capacity must: - be in the person’s ‘best interests’ (England and Wales) - have the potential to ‘benefit’ the person (Scotland)
Support for making decisions • Most people do not make important decisions in isolation • We recommend • Codes of Practice on mental capacity should be amended to emphasise • good communication • supportive relationships • joint decision making
Determining ‘best interests’ or ‘benefit’ • Past and present wishes of a person with dementia may sometimes conflict • Neither past nor present wishes can automatically take precedence • Important factors include: • the relative strength of the person’s wishes • the degree of importance of the decision • the amount of distress being caused • We conclude Extra guidance is needed on balancing thesefactors
Advance decisions • Advance decisions to refuse treatment are legally binding as long as they have been properly made • A welcome opportunity to exercise autonomy? • OR • Potentially harmful for future care decisions? • We conclude • It is right for the law to allow people to make an advance decision to refuse treatment if they wish to do so. However, an advance refusal of treatment may not always work in the way the person expected.
Advance care planning • May include: • Medical treatment • Wishes about where they would like to be as they are dying • Particular likes and dislikes • Who they would most want to be with them • We conclude • Decisions about future care are best achieved in the broader context of advance care planning
Welfare attorneys • People nominated to take health or welfare decisions on behalf of a person if, in the future, they lose capacity to make those decisions themselves • Must act in the best interests of the person with dementia • We conclude • Welfare attorneys are a ‘social good’ and the process of appointing a welfare attorney should be free of charge for everyone
Challenges to welfare attorneys • A welfare attorney may disagree with doctors over the best interests of the person with dementia, and such disputes can be referred to court • We recommend • More guidance is needed about when it is appropriate for professionals to challenge the decision of a welfare attorney in court • Significant weight should be placed on the fact that the welfare attorney was previously chosen and trusted by the person
Launch of the report • Dementia: ethical issues • 1 October 2009
Dementia: ethical issues • Dilemmas in care • Professor Julian Hughes • Consultant in Old Age Psychiatry and Honorary Professor of the Philosophy of Ageing, Northumbria Healthcare NHS Foundation Trust and Institute for Ageing and Health, Newcastle University
Overview • Ethical dilemmas arise on a daily basis • These are often stressful • Those providing care need more support in tackling these dilemmas • Guidelines are helpful, but not enough • We recommend • Those involved in direct care of people with dementia should have access to ongoing education and support in ethical decision making