Download
1 / 1
10 likes | 115 Views
No . 104 . Is Preoperative Mid-Stream Urine (MSU) Screening Worthwhile?. Renu Eapen, Yeng Kwang Tay, Francis Ting, Philip McCahy Department of Urology, Monash Medical Centre, Melbourne, Australia. Results Infection identified in 207 / 1004 (20.6%) patients

E N D
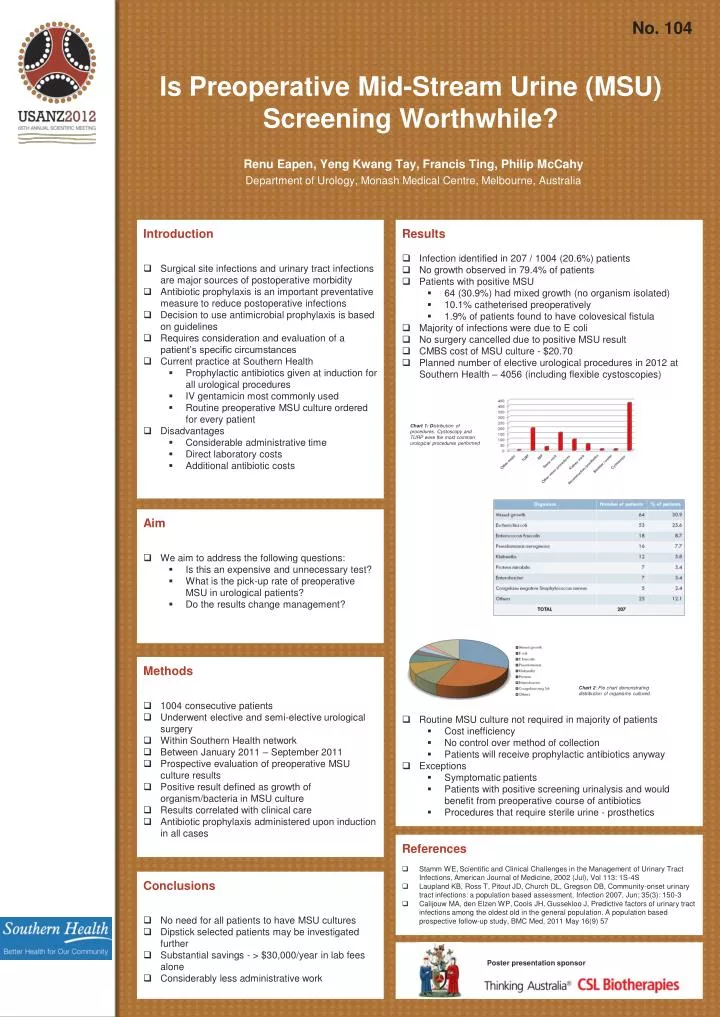
No. 104 Is Preoperative Mid-Stream Urine (MSU) Screening Worthwhile? Renu Eapen, Yeng Kwang Tay, Francis Ting, Philip McCahy Department of Urology, Monash Medical Centre, Melbourne, Australia • Results • Infection identified in 207 / 1004 (20.6%) patients • No growth observed in 79.4% of patients • Patients with positive MSU • 64 (30.9%) had mixed growth (no organism isolated) • 10.1% catheterised preoperatively • 1.9% of patients found to have colovesical fistula • Majority of infections were due to E coli • No surgery cancelled due to positive MSU result • CMBS cost of MSU culture - $20.70 • Planned number of elective urological procedures in 2012 at Southern Health – 4056 (including flexible cystoscopies) • Routine MSU culture not required in majority of patients • Cost inefficiency • No control over method of collection • Patients will receive prophylactic antibiotics anyway • Exceptions • Symptomatic patients • Patients with positive screening urinalysis and would benefit from preoperative course of antibiotics • Procedures that require sterile urine - prosthetics • Introduction • Surgical site infections and urinary tract infections are major sources of postoperative morbidity • Antibiotic prophylaxis is an important preventative measure to reduce postoperative infections • Decision to use antimicrobial prophylaxis is based on guidelines • Requires consideration and evaluation of a patient’s specific circumstances • Current practice at Southern Health • Prophylactic antibiotics given at induction for all urological procedures • IV gentamicin most commonly used • Routine preoperative MSU culture ordered for every patient • Disadvantages • Considerable administrative time • Direct laboratory costs • Additional antibiotic costs Chart 1: Distribution of procedures. Cystoscopy and TURP were the most common urological procedures performed • Aim • We aim to address the following questions: • Is this an expensive and unnecessary test? • What is the pick-up rate of preoperative MSU in urological patients? • Do the results change management? • Methods • 1004 consecutive patients • Underwent elective and semi-elective urological surgery • Within Southern Health network • Between January 2011 – September 2011 • Prospective evaluation of preoperative MSU culture results • Positive result defined as growth of organism/bacteria in MSU culture • Results correlated with clinical care • Antibiotic prophylaxis administered upon induction in all cases Chart 2: Pie chart demonstrating distribution of organisms cultured. • References • Stamm WE, Scientific and Clinical Challenges in the Management of Urinary Tract Infections, American Journal of Medicine, 2002 (Jul), Vol 113: 1S-4S • Laupland KB, Ross T, Pitout JD, Church DL, Gregson DB, Community-onset urinary tract infections: a population based assessment, Infection 2007, Jun; 35(3): 150-3 • Calijouw MA, den Elzen WP, Cools JH, Gussekloo J, Predictive factors of urinary tract infections among the oldest old in the general population. A population based prospective follow-up study, BMC Med, 2011 May 16(9) 57 • . • Conclusions • No need for all patients to have MSU cultures • Dipstick selected patients may be investigated further • Substantial savings - > $30,000/year in lab fees alone • Considerably less administrative work Poster presentation sponsor






