Download
1 / 36
360 likes | 527 Views
Comorbidities in an Aging HIV Positive Population. Fernando Garcia, MD Valley AIDS Council HalingenTExas. Comorbidities Associated With an Aging HIV Positive Population. I. Epidemiology II. Introduction to Case Study III. Comorbidities Renal Lipodystrophy

E N D
Comorbidities in an Aging HIV Positive Population Fernando Garcia, MD Valley AIDS Council HalingenTExas
Comorbidities Associated With anAging HIV Positive Population I. Epidemiology II. Introduction to Case Study III. Comorbidities • Renal • Lipodystrophy • Insulin Resistance / Diabetes • Cardiovascular IV. Case Study Facilitation
HAART & An Aging HIV Positive Population • The success of HAART has dramatically enhanced life expectancy among HIV positive individuals1 • By 2015, it is estimated that more than one-half of all HIV positive individuals in the US will be aged >50 years2 1Munoz A, et al. AIDS. 1997;11:S69-76. 2Statement from Senator Gordon H. Smith. Aging hearing: HIV over fifty, exploring the new threat. Available at: http://aging.senate.gov/events/hr141gs.pdf. Accessed September 25, 2008.
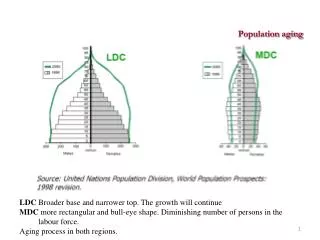
Age Distribution (in years) of HIV Positive Individuals Living in the United States Adapted from CDC Surveillance Report 2006
Rate of HIV Related Deaths Have Declined Since 1999 Overall deaths HIV-related deaths Non-HIV-related deaths Age-adjusted AIDS mortality rate by underlying cause of death 900 800 700 600 Rate per 10,000 persons with AIDS 500 400 300 200 100 1999 2000 2001 2002 2003 2004 Years • 1 out of 4 deaths of patients with AIDS was non-HIV related • The proportion of deaths due to non-HIV related causes increased over this time period Sackoff JE, et al. Ann Interm Med. 2006;145:397-406.
Comorbidities Associated with an Aging HIV Positive Population • Age related comorbidities are important in HIV positive individuals: • Renal1 • Lipodystrophy2 • Insulin Resistance / Diabetes3 • Cardiovascular4 • These comorbidities in HIV positive patients may be increasingly important in determining the course of therapy in an aging patient population 1Gupta SK, et al. Clinical Infectious Disease. 2005; 40:1559-1585., 2Falutz J., Nat Clin Pract Endocrinol Metab. 2007 Sep;3(9):651-61. 3Florescu, D. Antiretroviral Therapy. 2007. 12:149-162. 4Schambelan M et al. Circulation. 2008;118:e48-e53.
Comorbidities Associated With anAging HIV Positive Population I. Epidemiology II. Introduction to Case Study III. Comorbidities • Renal • Lipodystrophy • Insulin Resistance / Diabetes • Cardiovascular IV. Case Study Facilitation
Case Study: Treatment-Experienced Patient • Patient is a 63-year-old African American man who presents to the office for routine follow-up • HIV positive for 6 years and has been on a BID boosted PI-based antiretroviral regimen since diagnosis • No history of prior treatment intolerance or virologic failures • He describes mild long-standing fatigue and infrequent episodes of diarrhea • Current labs: • CD4+ = 436 cells/mm3, VL <50 copies/mL, • WBC = 5.2 cells/μL, Hgb = 14.1g/dL, Platelet count = 236,000 • TC = 212 mg/dL, TG = 190 mg/dL, LDL = 123 mg/dL, HDL = 41 mg/dL • FBG = 120mg/dl, Creatinine = 1.2 mg/dL, BUN = 6 mg/dL, Normal LFTs • eGFR (C-G method) = 78.8 mL/min/1.73 m2
Case Study: Treatment-Experienced Patient • Current meds: ARV regimen, statin, PRN antidiarrheal • No history of diabetes, HTN, tobacco use, or family history of CAD • Physical exam: lipoatrophy of face, arms, and legs; Waist circumference = 39” • Patient is starting a new job and has concerns about his current ARV regimen
Case Study: Treatment-Experienced Patient • How does this patient’s age affect your initial evaluation? • How do his physical exam and lab values factor into treatment decisions? • What are the similarities and differences in how you would manage this patient compared to a younger patient?
Comorbidities Associated With anAging HIV Positive Population I. Epidemiology II. Introduction to Case Study III. Comorbidities • Renal • Lipodystrophy • Insulin Resistance / Diabetes • Cardiovascular IV. Case Study Facilitation
Prevalence of Chronic Kidney Disease in the General Population Increases with Age Eight year cross-sectional Norwegian survey subjects ≥20 yrs of age GFR (mL/min/1.73 m2): 45 45-59 <30 30-44 N = 65,605 Prevalence (%) Age (Years) Adapted from Hallan SI, et al. BMJ. 2006; 333:1047-1050.
Renal Disease in HIV Positive Patients • Kidney disease is an important complication of HIV infection in the era of antiretroviral therapy1 • In a retrospective study of 487 consecutive HIV positive patients with normal renal function, the initial prevalence of CKD was 2%2 • After 5 years of follow-up, 6% had progressed to CKD • Older age was a multivariate predictor of CKD for this cohort 1Gupta SK, et al. Clinical Infectious Disease. 2005; 40:1559-1585.2Gupta SK, et al. Clinical Nephrology. 2004.; 61:1-6.
Kidney Disease in HIV Positive Patients • The spectrum of kidney disease in HIV includes: • HIV-associated nephropathy • Immune complex kidney disease • Medication nephrotoxicity • Kidney disease related to co-morbid conditions • Diabetes, hypertension, and hepatitis virus co-infection Wyatt, CM. AJM. 2007. 120;488-49.
Risk Factors for Kidney Disease in the HIV Positive Population Ethnicity Family History Age CKD Risk Hyper- tension HIV ART Diabetes Hepatitis C = Modifiable = Nonmodifiable Gupta SK, et al. Clinical Infectious Disease. 2005; 40:1559-1585.
IDSA Initial Evaluation Recommendations • Obtain baseline GFR: • All patients at the time of HIV diagnosis should be assessed for existing kidney disease with a screening urinalysis for proteinuria and a calculated estimate of renal function • Annual screening: • If there is no evidence of proteinuria at initial evaluation, patients at high risk for the development of proteinuric renal disease should undergo annual screening • Renal function should be estimated on a yearly basis to assess for changes over time • When to consider a nephrology consult: • Additional evaluations and referral to a nephrologist are recommended for patients with proteinuria of grade ≥1+ by dipstick analysis or GFR<60 mL/min per 1.73m2 Gupta SK, et al. Clinical Infectious Disease. 2005; 40:1559-1585.
Comorbidities Associated With anAging HIV Positive Population I. Epidemiology II. Introduction to Case Study III. Comorbidities • Renal • Lipodystrophy • Insulin Resistance / Diabetes • Cardiovascular IV. Case Study Facilitation
The Causation of Lipodystrophy Is Multi-Factorial in HIV Positive Patients
Potential Clinical Impact of Lipodystrophy • Morphological1 • Quality of life • Patient adherence • Metabolic2 • Insulin resistance • Impaired glucose tolerance • Type 2 diabetes • Hypertriglyceridemia • Hypercholesterolemia • Increased free fatty acids (FFA) • Decreased high density lipoprotein (HDL) 1Falutz J., Nat Clin Pract Endocrinol Metab. 2007 Sep;3(9):651-61. 2Behrens G, et al. Lipodystrophy syndrome. HIV Medicine. 15th ed. 2007. Available at: http://www.hivmedicine.com/hivmedicine2007.pdf. Accessed September 25, 2008.
Therapeutic Options for Managing Lipodystrophy • Lifestyle changes • Reduce saturated fat/ cholesterol intake • Increase physical activity • Cease smoking • Evaluate ARVs • Manage chronic co-morbid conditions • e.g. hypertension, hyperlipidemia, diabetes Falutz J., Nat Clin Pract Endocrinol Metab. 2007 Sep;3(9):651-61.
Comorbidities Associated With anAging HIV Positive Population I. Epidemiology II. Introduction to Case Study III. Comorbidities • Renal • Lipodystrophy • Insulin Resistance / Diabetes • Cardiovascular IV. Case Study Facilitation
Insulin Resistance and Diabetes in the HIV Positive Population • An increased prevalence of insulin resistance, glucose intolerance and diabetes has been reported in HIV infections in the HAART era1 • Diabetes in HIV positive men with HAART exposure > 4X HIV-seronegative men2 • Risk factors for HIV positive individuals developing diabetes include3: • Certain ARVs • Older age • Ethnic background (African American) • Male sex • Greater BMI 1Florescu, D. Antiretroviral Therapy. 2007. 12:149-162.2Brown, TT. Arch Intern Med. 2005. 165:1179-1184.3DeWit, D. Diabetes Care. 2008. 31(6):1224-1229.
Diabetes Diagnostic Criteria Florescu, D. Antiretroviral Therapy. 2007. 12:149-162.
Complications of Insulin Resistance • Insulin resistance occurs as part of a metabolic syndrome that may lead to the development of: • Type II diabetes • Atherosclerosis • Hypertension Florescu, D. Antiretroviral Therapy. 2007. 12:149-162.
Diagnosis and Management of InsulinResistance in HIV-Infected Patients • Fasting serum glucose measurement • At baseline and 3-6 months after starting HAART • Yearly thereafter • Oral glucose tolerance test • At the first visit in patients with family history of diabetes or obesity • Repeat when there is clinical suspicion of impaired glucose tolerance • Lifestyle modification • Diabetic education • Self-monitoring of blood glucose • Aerobic and resistance training Florescu, D. Antiretroviral Therapy. 2007. 12:149-162.
Comorbidities Associated With anAging HIV Positive Population I. Epidemiology II. Introduction to Case Study III. Comorbidities • Renal • Lipodystrophy • Insulin Resistance / Diabetes • Cardiovascular IV. Case Study Facilitation
Cardiovascular Disease in the HIV Positive Population • Cardiovascular (CV) disease has emerged as a health concern in the aging HIV-positive population as HAART can provide durable clinical benefit and improved survival • Contributes to more than 10% of deaths among HIV positive individuals • Factors that affect CV risk are similar for HIV positive and negative individuals • Risk may vary among ARV agents D:A:D Study Group. The Lancet. 2008. 371(9622):1417-26.
100 HIV+ 80 HIV– 60 Events per 1000 Person-Years 40 20 0 45-54 18-34 35-44 55-64 65-74 Age Group (Years) MI Rates in HIV Positive and HIV Negative Patients AMI rate by age group Cohorts (HIV+ =3851, HIV- =1,044,589) were identified in the Research Patient Data Registry. The primary outcome was AMI. Triant VA,et al. J Clin Endocrinol Metab. 2007;92:2506-2512.
= ART = HIV Infection = HIV Infection & ART HIV Related Factors that May Contribute to Cardiovascular Disease Persistent Inflammation Endothelial Dysfunction Lipid Disorders HAART Vascular Disease in HIV Positive Patients ART-Associated Lipodystrophy Insulin Resistance Viremia Oxidative Stress Adapted from Dube M, et al. Circulation. 2008;118:e36-e40.
IDSA Guidelines: General Approach to CV Risk in HIV Positive Patients Obtain fasting lipid profile, prior to starting antiretrovirals and within 3 to 6 months of starting new regimen Count number of CHD risk factors and determine level of risk.If ≥2 risk factors, perform a 10-year risk calculation Intervene for modifiable nonlipid risk factors, including diet and smoking If above the lipid threshold based on risk group despite vigorous lifestyle interventions, consider altering antiretroviral therapy or lipid-lowering drugs IF LIPID-LOWERING DRUGS ARE NECESSARY Serum LDL cholesterol above threshold, or triglycerides 200-500 mg/dL with elevated non-HDL cholesterol: STATINS Serum triglycerides >500 mg/dL:FIBRATES OR Dubé MP et al. Clin Infect Dis. 2003;37:613-627. IDSA = Infectious Diseases Society of America.
Calculating Framingham Risk Available at: http://hp2010.nhlbihin.net/atpiii/calculator.asp?usertype=prof. Accessed September 25, 2008.
Summary • Due to advances in HAART, HIV positive patients are growing older and living longer • HIV positive individuals may experience common comorbidities as they grow older • Renal dysfunction • Lipodystrophy • Insulin resistance / Diabetes • Cardiovascular disease • Comorbidities may be increasingly important in therapeutic decisions involving aging HIV positive patients
Comorbidities Associated With anAging HIV Positive Population I. Epidemiology II. Introduction to Case Study III. Comorbidities • Renal • Lipodystrophy • Insulin Resistance / Diabetes • Cardiovascular IV. Case Study Facilitation
Case Study: Treatment-Experienced Patient • Patient is a 63-year-old African American man who presents to the office for routine follow-up • HIV positive for 6 years and has been on a BID boosted PI-based antiretroviral regimen since diagnosis • No history of prior treatment intolerance or virologic failures • He describes mild long-standing fatigue and infrequent episodes of diarrhea • Current labs: • CD4+ = 436 cells/mm3, VL <50 copies/mL, • WBC = 5.2 cells/μL, Hgb = 14.1g/dL, Platelet count = 236,000 • TC = 212 mg/dL, TG = 190 mg/dL, LDL = 123 mg/dL, HDL = 41 mg/dL • FBG = 120mg/dl, Creatinine = 1.2 mg/dL, BUN = 6 mg/dL, Normal LFTs • eGFR (C-G method) = 78.8 mL/min/1.73 m2
Case Study: Treatment-Experienced Patient • Current meds: ARV regimen, statin, PRN antidiarrheal • No history of diabetes, HTN, tobacco use, or family history of CAD • Physical exam: lipoatrophy of face, arms, and legs; Waist circumference = 39” • Patient is starting a new job and has concerns about his current ARV regimen
Case Study: Treatment-Experienced Patient • How does this patient’s age affect your initial evaluation? • How do his physical exam and lab values factor into treatment decisions? • What are the similarities and differences in how you would manage this patient compared to a younger patient?