Download
1 / 14
140 likes | 265 Views
Have SWAPs influenced aid flows and aid effectiveness? Rohan Sweeney, Duncan Mortimer and David W. Johnston 14 th February 2014. www.buseco.monash.edu.au/centres/che /. “ SWAp has truly become a popular and widespread means of coordinating and structuring development aid”

E N D
Have SWAPs influenced aid flows and aid effectiveness? Rohan Sweeney, Duncan Mortimer and David W. Johnston 14th February 2014 www.buseco.monash.edu.au/centres/che/
“SWAp has truly become a popular and widespread means of coordinating and structuring development aid” (Sundewall and Sahlin-Andersson 2006).
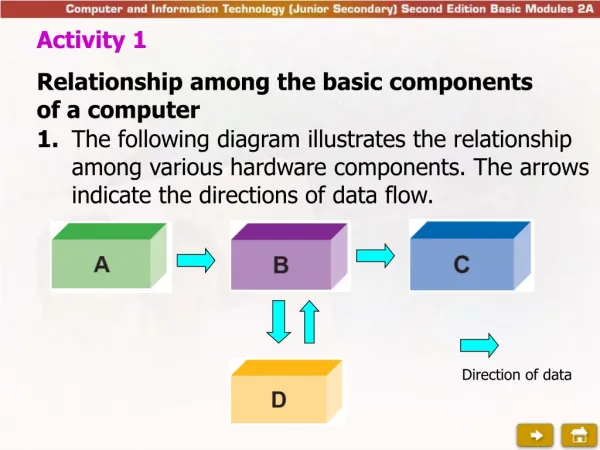
The SWAp is a “process rather than a fixed blueprint” (Walford 2003) Agreement Sector-wide health strategy Government-led Budgeted Share processes Government systems
SWAp has desired implications for DAH funding flows. • SWAp promotes increased general sector support. • SWAp can enable redirection of DAH towards domestic priority areas. Important because…. • Project-based DAH continues to dominate – only 7.7% sector support between 2002-06 (Piva and Dodd, 2009). • MDGs and disease focused donors (eg. GFATM, GAVI, Clinton) have encouraged disease specific project-based DAH. • Evaluations have found increases DAH support, however case study methods don’t enable contemporaneous control, so we can’t predict what would happen in absence of SWAp.
Impact of SWAp on funding flows - research questions • has DAH allocated to sector support increased as a result of SWAp implementation? • have SWAps changed how DAH has been allocated across other key health funding areas?
Methods • Searched for countries with implemented health SWAps. • Constructed a unique dataset of DAH recipient countries, which includes total levels of DAH and levels allocated between key health areas (IHME 2011): • HIV, TB, “maternal and child health (MNCH), malaria, sector support and NCDs. • Using a linear probability model, comparable treatment and control countries were identified. Likelihood of SWAp implementation was predicted given: • GDP/capita, DAH levels, geographic region, no. of donors, life expectancy, and population levels. • Fixed effect panel regression techniques employed.
The sample a t-test for difference in means with unequal variance.
^ Beta distributions Standard errors in parentheses * p < 0.10, ** p < 0.05, *** p < 0.01
Key messages • SWAps have facilitated increased levels of DAH directed as sector support. • SWAps appear to have facilitated reallocations of DAH fund flows across key health areas, specifically away from HIV and MNCH. • SWAp implementation has facilitated changes in funding flows consistent with SWAp aims to increase country ownership of DAH programmes.
References Brown A, Foster M, Norton A and Naschold F. The status of sector wide approaches. Centre for Aid and Public Expenditure. Working Paper 142. 2001. Overseas Development Institute. Institute for Health Metrics and Evaluation , I. (2011). Development Assistance for Health Country and Regional Recipient Level Database 1990-2009. Seattle, Institute for Health Metrics and Evaluation OECD Development Co-operation Directorate. (2010). "Paris Declaration and Accra Agenda for Action." Piva, P. and R. Dodd (2009). "Where did all the aid go? An in depth analysis of increased aid flows over the past 10 years." Bulletin of the World Health Organization 87: 930-939. RavishankarN, Gubbins P, Cooley RJ, Leach-Kemon K, Michaud CM, Jamison DT, Murray CJL. Financing of global health: tracking development assistance for health from 1990 to 2007. The Lancet 2009;373; 2113-2124 Sundewall J, Sahlin-Andersson K. Translations of health sector SWAps--a comparative study of health sector development cooperation in Uganda, Zambia and Bangladesh. Health Policy. 2006 May;76(3):277-87. Walt G, Pavignani E, Gilson L, Buse K. Health sector development: from aid coordination to resource management. Health Policy Plan. 1999(a);14:207–18. Walford, V. (2003). Defining and evaluating SWAps: a paper for the Inter-Agency Group on SWAps and Development
Appendix: model specifications Has sector DAH increased under SWAp? (1) sector_DAHit= αi + δSWApit-1 + β1malariait-1 + β2HIVit-1 + β3TBit-1+ β4IMRit-1 + β5log(GDP/capita)it-1 + β6gov_effect it-1 + β7corruptionit-1 + μt + εit Note: the impact on both absolute levels of Sector_DAH and also the proportion of total DAH allocated to the sector is estimated. Has SWAp changed allocations between other key health areas? (2) tb_DAHit= αi + δSWApit-1 + β1malariait-1 + β2HIVit-1 + β3TBit-1 + β4IMRit-1 + β5log(GDP/capita)it-1 + β6gov_effect it-1 + β7corruptionit-1 + μt + εit Comparable specifications estimated for DAH directed to HIV, malaria and MNCH. NCDs omitted due to lack of meaningful burden of disease control for full period.
^ Beta distributions Standard errors in parentheses * p < 0.10, ** p < 0.05, *** p < 0.01