Download
1 / 23
230 likes | 496 Views
Advanced Paramedic Skills. Fleming College Year 2- Paramedic Program Mary Osinga – A-EMCA , CCFP –BSc. 60 Hours of Fun and Excitement!. Standards and DMAs Advanced patient assessment Safety and professionalism ACR and Documentation of DMA’s Cardiac Monitoring, 12-Lead and AED

E N D
Advanced Paramedic Skills Fleming College Year 2- Paramedic Program Mary Osinga – A-EMCA , CCFP –BSc
Standards and DMAs • Advanced patient assessment • Safety and professionalism • ACR and Documentation of DMA’s • Cardiac Monitoring, 12-Lead and AED • Medication Administration • IV Therapy (Starts and Monitoring) • Working With Advanced Care Paramedics • ACP Drugs What are we covering?
Establish criteria for mandatory core requirement for paramedics from the Ministry of Health • Introduce the Provincial Base Hospital standards for Symptom Relief , Defibrillation, IV therapy for PCPs and 12/15 Lead • Introduce Regional requirements for local equipment, knowledge and practice • Familiarity with practical applications of the above • Make you competent! (and safe!) Focus of the Course
PCP • ACP • CCP • See Regulation 257 and KNOW how it applies to YOU! • Ambulance Act requirements for Paramedics Scope of Practise
Ambulance Act & Regulations • Health Care Consent Act • Regulated Health Professions Act • Child & Family Service Act • Coroner's Act • Health Protection & Promotion Act • Highway Traffic Act • Mental Health Act • PHIPA • Occupational Health & Safety Act Legal Requirements for Paramedics
Why? • Standards • Use of Protocols Advance Life Support Patient Care Standards V. 3.0
Protocols - Guidelines for prehospital patient care. Only the portion of the guidelines which are designated “medical directives" may be undertaken before contacting on-line medical control. • Standing orders - Advanced life support interventions which may be undertaken aftercontacting on line medical control • On-line medical control - Medical direction of prehospital ACP activities by direct radio or telephonic communications with an on-line medical control physician. • Standards- prescribed accepted medical treatment that is set by a governing body (E.g BLS standards) • See example Difference between Standards and Protocols
Example of Standing Order–components • E.g NTG • How they are written is CRITICAL!! • List the headings • A • B • C • D • E • Consent to Treatment/Refusal • Other Standards • Auxiliary Medical Directives Medical Directives
Two types • Implied – either given spontaneous-e.g hand outstretched or assumed (e.g. unconscious) that person would want to have treatment or procedure • Informed – requires discussion of procedures, risks, consequences and outcomes • See Aid to capacity evaulation Consent –Imperative to obtain
What does it mean to you? • Investigations branch of MOH • Code 7 Calls • Your requirements under Ambulance Act Maintenance of Certification Policy Appendix 6 ALSPCS Vs 3.1
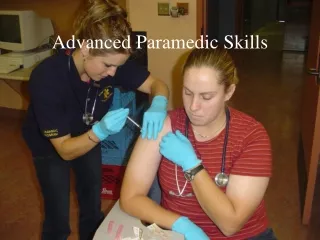
Medical protective gear is IMPERITIVE • Don’t become one of the statistics • Blood and body fluid contact IS part of the job. Minimize risk via • Gloves and/or double glove • Gowns for certain situations • Eyewear , goggles and face shield • Mask, surgical or N95 • Proper uniform adherence Medical PPE, Splash/Contact
an infection control principle that treats all human blood and other potentially infectious materials as infectious • The new normal after SARS! What is Universal Precautions?
What are sharps? In the prehospital environment? • IV catheters • End of IV tubing • Syringes for drugs such as glucagon, epinephrine, • Preloads (ALS) • Other drugs, Morphine, lasix, etc Sharps
Did the injury occur: • Before use 0% • During use 8% • Between steps 16% • Disassembling 0% • Preparing for reuse 0% • Recapping 0% • Withdrawing from resistant material 0% • Other after use, before disposal 59% • Item left on disposal container 0% • Putting item into disposal container16% • After disposal 0% • Pierced side of disposal container 0% • Pierced side of inappropriate disposal container 1 % • Restraining 0% • Other 6% HOW SHARP INJURYS OCCURRED
After performing phlebotomy on a patient with AIDS, a health care worker sustained a deep needlestick injury with the used phlebotomy needle. Blood from the collection tube also spilled into the space between the wrist and cuff of the health care worker's gloves, contaminating her chapped hands. The health care worker removed the gloves and washed her hands immediately. She had a negative baseline HIV test and refused zidovudine prophylaxis. Because her patient was not known to have HCV infection and did not have clinical evidence of liver disease, the health care worker did not receive baseline testing for exposure to HCV. Eight months after the incident, the health care worker was hospitalized with acute hepatitis. She was found to be seropositive for HIV 9 months after the incident. Sixteen months after the incident, she tested positive for anti-HCV antibodies and was diagnosed with chronic HCV infection. Her clinical condition continued to deteriorate, and she died 28 months after the needlestick injury [Ridzon et al. 1997 Serious Stuff
Risk –The risk of infection varies depending on the pathogen: HIV carries a 3% risk of transmission, 5% for Hep C , and 6%-30% for Hep B. • HBV infections among health care workers has declined dramatically over the last ten years, due to widespread immunization of healthcare workers with the hepatitis B vaccine, • Many factors will affect transmission of pathogens • Type of needle used (gauge) • Pre-post patient contact • Depth of stick injury • Muscle vs sub cut vs scratch • Post needle stick care Needle Stick Injuries
Comply with universal precautions • Minimize exposure or risk • Necessary procedure? • Use of safer devices such as needleless • Prohibition of recapping, or removing contaminated needles • Training in appropriate engineering controls and work practices • Post-exposure evaluation and follow-up, including post-exposure prophylaxis when appropriate Needle Stick InjuriesPrevention
Move towards making systems needle-less • These devices take a while to get used to for health care workers who are used to needle • Greatly reduce risk when used properly • IV catheters, syringes are most commonly seen in the prehospital environment Needles vs Needle-less!
Blunt tip Safety Safety Safety catheter
Be professional when using needles, syringes • Prepare your equipment • Have sharps container nearby and ready • Know how equipment works • Anticipate patient movement • Move slowly, haste makes extra holes! • ALWAYS dispose of sharp IMMEDIATELY after use • Know reporting procedure for injuries • Wash immediately after injury with soap and water, get assessment From a medic point of view
Readings • Safety 2 • Ready Introduction to ALS PCS V 3.1 • Look At PCP Handbook -CEPCP • READ Defib protocols ALS PCS • Cardiac Arrest 27.72-end chapter 27 Scenario: You are driving to the cottage, when you come across an accident. There is a 7yr old boy lying on the road, ejected from the vehicle. He has a pulse but no respirations. What do you do? What protection will you use if there is blood in the airway? Be Safe!