Download
1 / 27
410 likes | 2.44k Views
Erythrocytosis (Polycythemia). 22 Nov 2009. Polycythaemia. Polycythaemia (erythrocytosis) is defined as an increase in the haemoglobin concentration above the upper limit of normal for the patient's age and sex. Classification of polycythaemia. Relative vs Absolute Absolute erythrocytosis

E N D
Erythrocytosis(Polycythemia) 22 Nov 2009
Polycythaemia Polycythaemia (erythrocytosis) is defined as an increase in the haemoglobin concentration above the upper limit of normal for the patient's age and sex.
Classification of polycythaemia • Relative vs Absolute • Absolute erythrocytosis • Hct male > 60%, female > 55%
Erythrocytosis (Polycythemia) I. Relative or spurious erythrocytosis Relative polycythemia is an apparent rise of the erythrocyte level in the blood; however, the underlying cause is reduced blood plasma. • Dehydration: water deprivation, vomiting • Plasma loss: burns, enteropathy II. Absolute erythrocytosis • Primary marrow diseases: PV,1ry erythrocytosis • Secondary : increased EPO production
Erythrocytosis • Reactive (Secondary ) : increased EPO production • Tissue hypoxia • Lung diseases : COPD • Heart disease: Rt to Lt shunt • High attitude • Abnormal Hb, smoking • Tumors produce EPO • Hypernephroma • Hepatoma • Cerebellar hemangioblastoma • Uterine fibromyoma • Renal diseases • Polycystic kidney • Renal artery stenosis
Polycythemia Vera (PV) Malignant clonal proliferation of hematopoietic stem cells leading to excessive erythrocyte production characterized as a panhyperplastic, malignant, and neoplastic marrow disorder. The increase in RBC mass occurs independent of erythropoietin. The median survival with treatment is about 9 to 14 years.
Frequency Polycythemia vera (PV) is relatively rare, occurring in 0.6-1.6 persons per million population.
Polycythemia vera Increase RBC production independent of normal mechanisms Median age 60 years Mutation of Janus 2 kinase gene (JAK2 V617F) Panmyelosis
Pathogenesis Disease Thrombosis
JAK2 mutation • Reported in 2005 • Mutation: JAK2V617F • Valine to Phenylalanine • Codon 617 • Myeloprolifertive disorders • PV 90-95% • ET 50-70% • MF 40-50%
Pathogenesis Thrombosis • High Hct • Platelet • No correlation with platelet count • Platelet defect • Increase platelet thromboxane A2 production • Decrease response prostaglandin D2 • Abnormal in vivo activation of leukocyte, endothelial cell • Decrease natural anticoagulant • Decrease fibrinolytic activity
Diagnostic criteria set by the PVSG are as follows: • Category A • Total red blood cell mass - In males, greater than or equal to 36 mL/kg; in females, greater than or equal to 32 mL/kg • Arterial oxygen saturation greater than or equal to 92% • Splenomegaly • Category B • Thrombocytosis with platelet count greater than 400,000/μL • Leukocytosis with a white blood cell count greater than 12,000/μL • Increased leukocyte alkaline phosphatase (ALP) greater than 100 U/L • Serum vitamin B-12 concentration greater than 900 pg/mL or binding capacity greater than 2200 pg/mL • The diagnosis is established with A1 plus A2 plus A3 or A1 plus A2 plus any 2 criteria from category B
Serum erythropoietin Low High Normal PV diagnosis probable PV diagnosis possible Evaluate for secondary polycythemia Bone marrow examination • Specialized tests • -JAK2 mutation • BM immunochemistry for c-mpl • PCR for PRV-1 gene • EEC formation Characteristics for PV? yes no PV Specialized test Mayo Clin Proc 2003;78:174-94. Reevaluate in 3 mo Consistent with PV Not consistent with PV
Clinical features • Physical Findings Frequency (%) • Symptoms Headache 48 Fatigue 47 Pruritus 43 Dizziness 43 Visual disturbances 31 Weight loss 29 Erythromelalgia 29 Dyspnea 26 Joint symptoms 26 Epigastric discomfort 24 thrombosis 20 • Signs Splenomegaly 70 Skin plethora 67 Conjunctival plethora 59 Engorged vessels in the optic fluid 46 Hepatomegaly 40 Systolic blood pressure > 140 mmHg 72 Diastolic blood pressure > 90 mmHg 32 Semin Haematol 1975;12:339-51
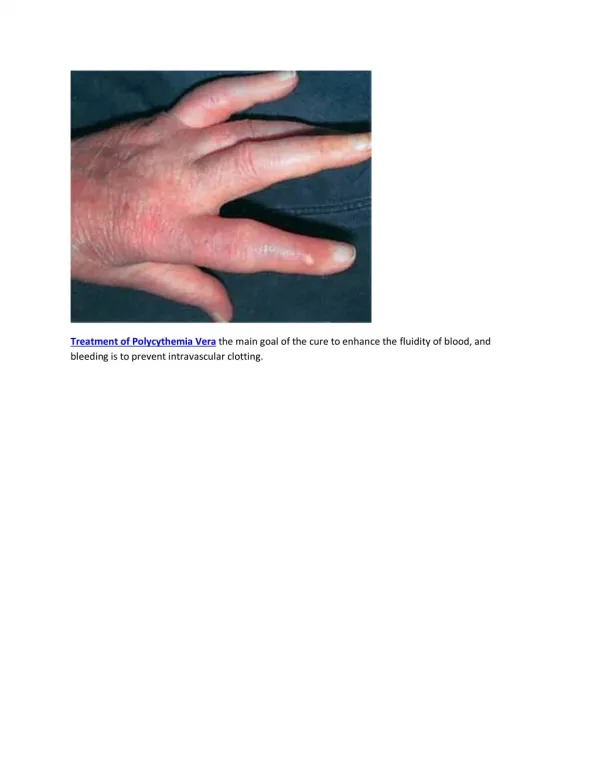
Erythromelalgia • Burning pain in the feet or hands accompanied by • erythema, pallor, or cyanosis • Microvascular thrombosis
Laboratory CBC Peripheral blood smear Bone marrow examination EPO level JAK2 mutation
CBC Red cell Increase Hct, Hb Not increase in PV with iron deficiency White cell Leukocytosis Band form, metamyelocyte, myelocyte (Lt shift) Increase basophil, eosinophil Platelet Increase or normal
Blood smear RBC: excess red cells, NC, NC hypochromic microcytic red cells (iron deficiency) WBC: increase with band form, myelocyte ,metamyelocyte Platelet: increase
Bone marrow smear Hypercellular marrow Increase erythroid, myeloid, megakaryocyte (panmyelosis) Normal maturation of myeloid series M:E = 2-3:1 Increase megakaryocytes with different size Negative iron stain
Cause of death • Cause of death • Thrombosis • Malignancy : acute leukemia, non-RE malignancy • Myelofibrosis • Bleeding
Risk of thrombosis • Old age: age > 60 years • Previous thrombosis • Phlebotomy treated group • Other cardiovascular disease: • DM • Smoking
Polycythemia Vera Phlebotomy to maintain Hct < 45% male, <42% female Low dose ASA • high risk of thrombosis • Age>60 years • Previous thrombosis • Other cardiovascular risk • Platelet > 1,500,000 /um Age 50-70 yr Age > 70 yr Age < 50 yr Busulphan or 32P Interferon Hydroxyurea
Clue diagnosis PV High Hct, absent secondary erythrocytosis Headache, plethora, thrombosis, pruritus Mild to moderate splenomegaly Hepatomegaly Leukocytosis, thrombocytosis Panmyelosis Low erythropoietin level JAK2 mutation