Download
1 / 1
10 likes | 137 Views
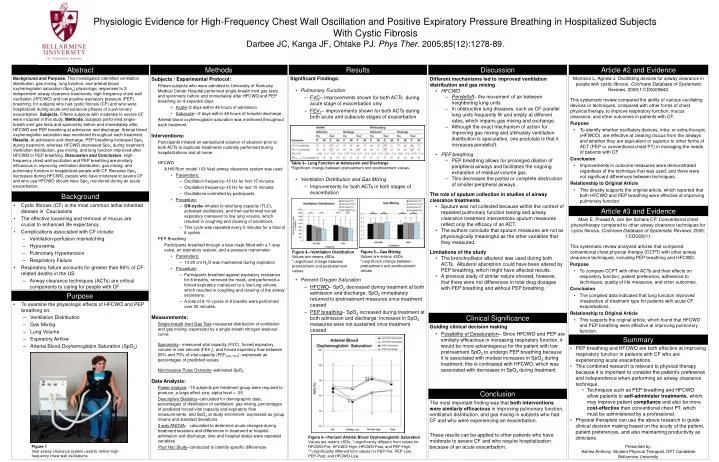
Figure 1 Vest airway clearance system used to deliver high-frequency chest wall oscillations.

E N D
Figure 1 Vest airway clearance system used to deliver high-frequency chest wall oscillations. Physiologic Evidence for High-Frequency Chest Wall Oscillation and Positive Expiratory Pressure Breathing in Hospitalized Subjects With Cystic FibrosisDarbee JC, Kanga JF, Ohtake PJ. Phys Ther. 2005;85(12):1278-89. Abstract Methods Results Discussion Article #2 and Evidence • Significant Findings: • Pulmonary Function • FVC– improvements shown for both ACTs during acute stage of exacerbation only • FEV1– improvements shown for both ACTs during both acute and subacute stages of exacerbation • Ventilation Distribution and Gas Mixing • Improvements for both ACTs in both stages of exacerbation • Percent Oxygen Saturation • HFCWO– SpO2 decreased during treatment at both admission and discharge; SpO2 immediately returned to pretreatment measures once treatment ceased • PEP breathing– SpO2 increased during treatment at both admission and discharge; increases in SpO2 measures were not sustained once treatment ceased • Morrison L, Agnew J. Oscillating devices for airway clearance in people with cystic fibrosis. Cochrane Database of Systematic Reviews. 2009;1:CD0006842. • This systematic review compared the ability of various oscillating devices or techniques, compared with other forms of chest physical therapy, to improve respiratory function, mucus clearance, and other outcomes in patients with CF. • Purpose • To identify whether oscillatory devices, intra- or extra-thoracic (HFWCO), are effective at clearing mucus from the airways and whether they are equivalent or superior to other forms of ACT (PEP or conventional chest PT) in managing the needs of patients with CF. • Conclusion • Improvements in outcome measures were demonstrated regardless of the technique that was used, and there were not significant differences between techniques. • Relationship to Original Article • This directly supports the original article, which reported that both HFCWO and PEP breathing were effective at improving pulmonary function. Background and Purpose. This investigation identified ventilation distribution, gas mixing, lung function, and arterial blood oxyhemoglobin saturation (Spo2) physiologic responses to 2 independent airway clearance treatments, high-frequency chest wall oscillation (HFCWO) and low positive expiratory pressure (PEP) breathing, for subjects who had cystic fibrosis (CF) and who were hospitalized during acute and subacute phases of a pulmonary exacerbation. Subjects. Fifteen subjects with moderate to severe CF were included in this study. Methods. Subjects performed single-breath inert gas tests and spirometry before and immediately after HFCWO and PEP breathing at admission and discharge. Arterial blood oxyhemoglobin saturation was monitored throughout each treatment. Results. At admission and discharge, PEP breathing increased Spo2 during treatment, whereas HFCWO decreased Spo2 during treatment. Ventilation distribution, gas mixing, and lung function improved after HFCWO or PEP breathing. Discussion and Conclusion. High-frequency chest wall oscillation and PEP breathing are similarly efficacious in improving ventilation distribution, gas mixing, and pulmonary function in hospitalized people with CF. Because Spo2 decreases during HFCWO, people who have moderate to severe CF and who use HFCWO should have Spo2 monitored during an acute exacerbation. . • Different mechanisms led to improved ventilation distribution and gas mixing • HFCWO • Pendelluft– the movement of air between neighboring lung units. • In obstructive lung diseases, such as CF, parallel lung units frequently fill and empty at different rates, which impairs gas mixing and exchange. • Although the exact mechanism of action for improving gas mixing and ultimately ventilation distribution is speculative, one postulate is that it increases pendelluft. • PEP breathing • PEP breathing allows for prolonged dilation of peripheral airways and facilitates the ongoing exhalation of residual volume gas. • This decreases the partial or complete obstruction of smaller peripheral airways . • The role of sputum collection in studies of airway clearance treatments • Sputum was not collected because within the context of repeated pulmonary function testing and airway clearance treatment interventions sputum measures reflect only the efficacy of an ACT. • The authors conclude that sputum measures are not as physiologically meaningful as the other variables that they measured. • Limitations of the study • The bronchodilator albuterol was used during both ACTs. Albuterol absorption could have been altered by PEP breathing, which might have affected results. • A previous study of similar nature showed, however, that there were not differences in total drug dosages with PEP breathing and without PEP breathing. • Subjects / Experimental Protocol: • Fifteen subjects who were admitted to University of Kentucky Medical Center Hospital performed single-breath inert gas tests and spirometry before and immediately after HFCWO and PEP breathing on 4 separate days: • Acute–2 days within 48 hours of admission • Subacute—2 days within 48 hours of hospital discharge Arterial blood oxyhemoglobin saturation was monitored throughout each treatment. Interventions: Participants inhaled an aerosolized solution of albuterol prior to both ACTs to duplicate treatments routinely performed during hospitalizations and at home. HFCWO • A Hill-Rom model 103 Vest airway clearance system was used • Parameters: • Oscillation frequency–10 Hz for first 15 minutes • Oscillation frequency–15 Hz for last 15 minutes • Oscillations controlled by participants • Procedure: • Off-cycle–inhaled to total lung capacity (TLC), activated oscillations, and then performed forced expiratory maneuver to low lung volume, which resulted in coughing and clearing of secretions. • This cycle was repeated every 5 minutes for a total of 6 cycles. • PEP Breathing • Participants breathed through a face mask fitted with a 1-way valve, an expiratory resistor, and a pressure manometer • Parameters: • 10-20 cm H2O was maintained during expiration • Procedure: • Participants breathed against expiratory resistance for 8 breaths, removed the mask, and performed a forced expiratory maneuver to a low lung volume, which resulted in coughing and clearing of the airway secretions. • A total of 8-10 cycles of 8 breaths were performed over 30 minutes. • Measurements: Single-breath Inert Gas Test–measured distribution of ventilation and gas mixing; expressed by a single breath nitrogen washout curve. Spirometry– measured vital capacity (FVC), forced expiratory volume in one second (FEV1), and forced expiratory flow between 25% and 75% of vital capacity (FEF25%-75%); expressed as percentages of predicted values. Noninvasive Pulse Oximetry–estimated SpO2 Data Analysis: Power analysis –15 subjects per treatment group were required to produce a large effect size, alpha level = .05 Descriptive Statistics–calculated for demographic data, percentages of distribution of ventilation, gas mixing, percentages of predicted forced vital capacity and expiratory flow measurements, and SpO2 at study enrollment; expressed as group means and standard deviations 3-way ANOVA– calculated to determine acute changes during treatment sessions and differences in treatment at hospital admission and discharge; time and hospital status were repeated variables Post Hoc Study–conducted to identify specific differences Table 3– Lung Function at Admission and Discharge bSignificant change between pretreatment and posttreatment values. Background • Cystic fibrosis (CF) is the most common lethal inherited disease in Caucasians • The effective loosening and removal of mucus are crucial to enhanced life expectancy. • Complications associated with CF include: • Ventilation-perfusion mismatching • Hypoxemia • Pulmonary Hypertension • Respiratory Failure • Respiratory failure accounts for greater than 80% of CF-related deaths in the US • Airway clearance techniques (ACTs) are critical components to caring for people with CF Article #3 and Evidence • Main E, Prasad A, van der Schans CP. Conventional chest physiotherapy compared to other airway clearance techniques for cystic fibrosis. Cochrane Database of Systematic Reviews. 2005; 1:CD002011. • This systematic review analyzed articles that compared conventional chest physical therapy (CCPT) with other airway clearance techniques, including PEP breathing and HFCWO. • Purpose • To compare CCPT with other ACTs and their effects on respiratory function, patient preference, adherence to techniques, quality of life measures, and other outcomes. • Conclusion • The compiled data indicated that lung function improved irrespective of treatment type for patients with acute CF exacerbations. • Relationship to Original Article • This supports the original article, which found that HFCWO and PEP breathing were effective at improving pulmonary function. Figure 5—Gas Mixing Values are means ±SDs. *=significant change between pretreatment and posttreatment values Figure 4—Ventilation Distribution Values are means ±SDs. *=significant change between pretreatment and posttreatment values Purpose • To examine the physiologic effects of HFCWO and PEP breathing on: • Ventilation Distribution • Gas Mixing • Lung Volume • Expiratory Airflow • Arterial Blood Oxyhemoglobin Saturation (SpO2) Clinical Significance • Guiding clinical decision making • Possibility of Desaturation– Since HFCWO and PEP are similarly efficacious in increasing respiratory function, it would be more advantageous for the patient with low pretreatment SpO2 to undergo PEP breathing because it is associated with modest increases in SpO2 during treatment; this is contrasted with HFCWO, which was associated with decreases in SpO2 during treatment. Summary • PEP breathing and HFCWO are both effective at improving respiratory function in patients with CF who are experiencing acute exacerbations. • This combined research is relevant to physical therapy because it is important to consider the patient’s preference and independence when performing an airway clearance technique. • Techniques such as PEP breathing and HFCWO allow patients to self-administer treatments, which may improve patient compliance and also be more cost-effective than conventional chest PT, which must be administered by a professional. • Physical therapists can use the above research to guide clinical decision making based on the acuity of the patient, patient preferences, and also maintaining productivity as clinicians. • Presented by: • Ashlea Anthony, Student Physical Therapist, DPT Candidate • Bellarmine University Conclusion The most important finding was that both interventions were similarly efficacious in improving pulmonary function, ventilation distribution, and gas mixing in subjects who had CF and who were experiencing an exacerbation. These results can be applied to other patients who have moderate to severe CF and who require hospitalization because of an acute exacerbation. Figure 6—Percent Arterial Blood Oxyhemoglobin Saturation Values are means ±SDs. *=significantly different from values for HFCWO-Pre, HFCWO-High, HFCWO-Post, and PEP-High. **=significantly different from values for PEP-Pre, PEP-Low, PEP-Post, and HFCWO-Low.



![Respiratory Physiology [the Ins and Outs]](https://cdn2.slideserve.com/4330665/respiratory-physiology-the-ins-and-outs-dt.jpg)