Download
1 / 102
1.02k likes | 1.08k Views
Renal Scintigraphy. Materials for medical students. Helena Balon, MD Wm. Beaumont Hospital Royal Oak, Michigan Charles University 3rd School of Medicine Dept Nucl Med, Prague. Renal perfusion and function Obstruction (Lasix renal scan) Renovascular HTN (Captopril renal scan)

E N D
Renal Scintigraphy Materials for medical students Helena Balon, MD Wm. Beaumont Hospital Royal Oak, Michigan Charles University 3rd School of Medicine Dept Nucl Med, Prague
Renal perfusion and function Obstruction (Lasix renal scan) Renovascular HTN (Captopril renal scan) Infection (renal morphology scan) Pre-surgical quantitation (nephrectomy) Renal transplant Congenital anomalies, masses (renal morphology scan) Indications Evaluation of:
Renal Function • Blood flow- 20% cardiac output to kidneys (1200 ml/min blood, 600 ml/min plasma) • Filtration - 20% renal plasma flow filtered by glomeruli (120 ml/min, 170 L/d) • Tubular secretion • Tubular reabsorption (1% ultrafiltrate - urine) • Endocrine functions
Renal RadiotracersExcretion Mechanisms GF TS TFTc-99m DTPA >95% Tc-99m MAG3 <5% 95% I-131 OIH 20% 80% Tc-99m GHA 40%-60% 20% Tc-99m DMSAsome 60% Semin NM Apr.92
Renal Radiopharmaceuticals Extract. fractionClearance Tc-99m DTPA 20% 100-120 ml/min Tc-99m MAG3 40-50% ~ 300 ml/min I-131 OIH ~100% 500-600 ml/min
Renal RadiopharmaceuticalsDosimetry DTPA MAG3 GHA DMSA I-131OIH rad/10 mCirad/5mCi rad/300µCi Kidney 0.2 0.15 1.6 3.5 0.01 Bladder 2.85.1 2.7 0.3 0.3 EDE (rem) 0.3 0.4 0.4 0.3 0.03
Perfusion MAG3, DTPA, GHA Morphology DMSA, GHA Obstruction MAG3, DTPA, OIH Relative function All GFR quantitation I-125 iothalamate, Cr-51 EDTA, DTPA ERPF quantitation MAG3, OIH Choosing Renal Radiotracers Clin. Question Agent
Basic Renal ScintigraphyPatientPreparation • Patient must be well hydrated • Give 5-10 ml/kg water (2-4 cups) 30-60 min. pre-injection • Can measure U - specific gravity (<1.015) • Void before injection • Void @ end of study Int’l Consens. Comm. Semin NM ‘99:146-159
Basic Renal ScintigraphyAcquisition • Supine position preferred • Do not inject by straight stick • Flow (angiogram) : 2-3 sec / fr x 1 min • Dynamic: 15-30 sec / frame x 20-30 min (display @ 1-3 min/frame)
Basic Renal ScintigraphyAcquisition (cont’d) • Obtain a 30-60 sec. image over injection site @ end of study • if infiltration >0.5% dose do not report clearance • Obtain post-void supine image of kidneys @ end of study Taylor, SeminNM 4/99:102-127
International Consensus Committee Recommendations for Basic Renogram • Tracer: MAG3, (DTPA) • Dose: 2 - 5 mCi adult, minimum 0.5 mCi peds • Pt. position: supine (motion, depth issues) • Include bladder, heart • Collimator: LEAP • Image over injection site Int’l Consens. Comm. Semin NM ‘99:146-159
Relative uptake • Contribution of each kidney to the total fct net cts in Lt ROI % Lt kid = --------------------------------------- x 100% net cts Lt + net cts Rt ROI • Normal 50/50 - 56/44 • Borderline 57/43 - 59/41 • Abnormal > 60/40 Taylor, SeminNM Apr 99
Basic Renal ScintigraphyProcessing • Time to peak • Best from cortical ROI • Normal < 5 min • Residual Cortical Activity (RCA20 or 30) • Ratio of cts @ 20 or 30 min / peak cts • Use cortical ROI • Normal RCA20 for MAG3 < 0.3 • Residual Urine Volume • (post-void cts x void. vol) (pre-void cts - post void cts)
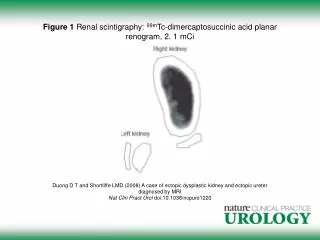
DTPA flow + scan GFR = 29 ml/’ Creat = 2.0 L= 33% R= 67%
Renogram Phases • I. Vascular phase (flow study): Ao-to-Kid ~ 3” • II. Parenchymal phase (kidney-to-bkg): Tpeak < 5’ • III. Washout (excretory) phase
Evaluation of Hydronephrosis Diuretic (Lasix) Renal Scan
Obstruction Obstruction to urine outflow leads to obstructive uropathy(hydronephrosis, hydroureter) andmay lead to obstructive nephropathy(loss of renal function)
Diuretic Renal ScanPrinciple • Hydronephrosis - tracer pooling in dilated renal pelvis • Lasix induces increased urine flow • If obstructed >>> will not wash out • If dilated, non-obstructed >>> will wash out • Can quantitate rate of washout (T1/2)
Diuretic Renal ScanIndications • Evaluate functional significance of hydronephrosis • Determine need for surgery • obstructive hydronephrosis - surgical Rx • non-obstructive hydronephrosis - medical Rx • Monitor effect of therapy
Diuretic Renal ScanRequirements • Rapidly cleared tracer • Well hydrated patient • Good renal function
Diuretic Renal ScanProcedure • Pt. preparation: • prehydration adults - oral or 360ml/m2 iv over 30’ peds - 10-15 ml/kg D5 0.3-0.45%NS • void before injection • bladder catheterization ?
Diuretic Renal ScanProcedure (cont’d) • Tracers: Tc-99m MAG3 5-10 mCi (preferred over DTPA) • Acquisition: supine until pelvis full (can switch to sitting post- Lasix) • Flow (angiogram) : 2-3 sec / fr x 1 min • Dynamic: 15-30 sec / frame x 20-30 min
Diuretic Renal ScanProcedure (cont’d) • Void before Lasix • Lasix: 40mg adult, 1mg/kg child iv @ ~10-20 min (when pelvis full)or @ -15min (“F-15” method) • Acquisition for 30 min post Lasix • Assess adequacy of diuresis • Measure voided volume • Adults produce ~200-300 ml urine post-Lasix
Diuretic Renal ScanProcedure (cont’d) • Don’t give Lasix if • Collecting system still filling • Collecting system not full by 60 min • Collecting system drains spontaneously • Poor ipsilateral fct (< 20%)
No UPJ obstruction T1/2 R = 6’ L = 2’
Pre-Lasix 10 y/o M
Rt UPJ obstruction T1/2 R = N/A F/U - nephrostomy tube placed
Lt hydronephrosis 3-wk old baby 3164897
Lt UPJ obstruction 3164897
Rt UPJ obstruction T1/2 R = N/A F/U - nephrostomy tube placed
Lt UPJ obstruction 3164897
Diuretic Renal ScanProcessing • ROI placement • around whole kidney or • around dilated renal collecting system • T/A curve • T1/2 • from Lasix injection vs. from diuretic response • linear vs. exponential fit of washout curve
Diuretic Renal ScanWashout(diuretic response) T1/2time required for 50% tracer to leave the dilated unit i.e. time required for activity to fall to 50% of peak
T1/2 washout cts 100% 50% T1/2 min
T1/2 value • Variables influencing T1/2 value: • Tracer • State of hydration • Volume of dilated pelvis • Bladder catheterization • Dose of Lasix • Renal function (response to Lasix) • ROI (kidney vs. pelvis) • T1/2 calculation (from inj. vs. response, curve fit)
T1/2 • Normal < 10 min • Obstructed > 20 min • Indeterminate 10 - 20 min • Best to obtain own normals for each institution, depending on protocol used
Diuretic Renal ScanInterpretation • Interpret whole study, not T1/2 alone • Visual (dynamic images) • Washout curve shape (concave vs. convex) • T1/2
Diuretic Renal ScanPitfalls • False positive for obstruction • Distended bladder • Gross hydronephrosis T(transit time) = V (volume) F (flow) • Poorly functioning / immature kidney • Dehydration • False negative • Low grade obstruction • Poorly functioning / immature kidney
Effect of catheterization (1) full bladder,no catheter