Download
1 / 31
310 likes | 331 Views
Learn about the global epidemiology of TB, the DOTS strategy for TB control, and the case definitions used to prioritize treatment and evaluate outcomes. Understand how TB is transmitted and the risk factors for progression to active TB.

E N D
Learning Objectives • Part 1 • Describe TB global epidemiology • Explain 5-point DOTS strategy for effective TB control • Understand TB case definitions • Part II • Explain how TB is transmitted • Describe active vs. latent TB • List risk factors for progression to active TB
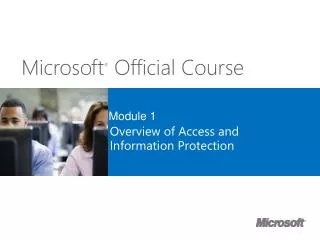
Estimated TB Incidence Rates, 2003 per 100 000 pop < 10 10 - 24 25 - 49 50 - 99 100 - 299 300 or more No estimate Global Epidemiology
HIV Prevalence in Adults, 2003 Adult prevalence % 15.0% − 39.0% 5.0% − 15.0% 1.0% − 5.0% 0.5% − 1.0% 0.1% − 0.5% 0.0% − 0.1% not available 38 million people [range: 35-42 million] living with HIV as of end 2003 UNAIDS Report on the Global HIV/AIDS Epidemic, 2004
Botswana Zimbabwe Malawi Tanzania Ivory Coast HIV Is Changing Global TB Epidemiology 700 600 500 400 Reported Case Rate (per 100,000) 300 200 100 0 1980 1983 1986 1989 1992 1995 1998 2001
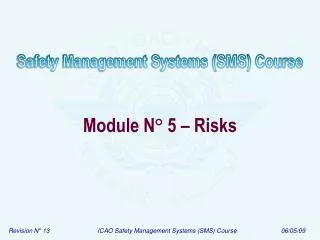
40 600 500 30 400 20 300 200 10 100 0 0 1975 1980 1985 1990 1995 2000 Reported TB Case Rate in Botswana, 1975–2002, and HIV Prevalence in Antenatal Women, 1992-2003 700 TB case rate (per 100,000) HIV seroprevalence (%)
Strategy and Framework Botswana and DOTS
TB Treatment--DOTS Strategy • Sustained • Government Commitment • to TB control 2. Microscopy-based Case Identification 3. Standardized Short Course Chemotherapy Under DOT 4. Secure Supply of Quality Drugs 5. Case Registry, Monitoring & Evaluation 2HRZE(S)/4HR
“Enhanced DOTS” • TB/HIV • MDR TB • Community TB Care • Private Public Mix (PPM)
What is the of DOTS? CASE DEFINITIONS HOLD THE PROGRAM TOGETHER
Case Definitions • Purposes • Proper patient registration and case notification • Prioritize treatment of smear-positive cases (the main source of infection in community) • Ensure cases on appropriate standardized regimens • Evaluate cases according to site of disease, bacteriology and treatment history • Permit cohort analysis of treatment outcomes
Matching diagnostic category and treatment regimens: Why? • Avoid under-treatment of previously diagnosed cases • Maximize cost-effective use of resources and minimize side effects by avoiding over-treatment
Determining the Case Definition • Four factors • Disease Classification (i.e., is site of disease (pulmonary, extrapulmonary or both?) • Bacteriology (i.e., smear status) • Patient Category ( determined by TB history—i.e., is patient “new” or “retreatment”?) • Severity of TB disease (cavitary vs. non-cavitary) First three factors recorded inregister
Disease Classification and Smear-Status: PTB+ vs. PTB- • PTB+ (Pulmonary TB smear-positive) • One AFB-positive smear; i.e. any patient with at least one positive smear result (irrespective of quantity of AFBs seen on microscopy) • Recommendations to improve the diagnosis of smear negative pulmonary and extrapulmonary TB among adults in HIV prevalent and resource constrained settings. • Draft for discussion by Strategic and Technical Advisory Group of Stop TB Department of WHOJune 2006
Site of Disease: PTB+ vs. PTB- • PTB- (smear-negative) Any pulmonary TB case that does not meet the definition of being smear-positive. This includes: 1. Patients with three negative smear results and radiological findings and doctor’s decision to treat for TB 2. Patients with negative smear results and a positive culture result for M. tuberculosis 3. Patients who are unable to produce sputum and with highly suspicious radiological and clinical findings and doctor's decision to treat for TB
Severity of Disease • Determinants include • Bacillary load • Extent of disease • Anatomical site • Significant acute threat to life (e.g., pericardial dx) • Risk of severe handicap (e.g., spinal TB) • Or both (e.g., meningitis) • Miliary considered severe • EPTB can be “severe” or “less severe”
Registration Category: New Determined by previous treatment history NEW: Never had TB treatment or who has taken anti-TB treatment (ATT) < 1 month RETREATMENT (3 types): Any patient who has taken > 1 month of ATT
Registration Category: Retreatment RETREATMENT CASES RELAPSE: A patient previously treated for TB who has been declared cured or treatment completed, and is diagnosed with bacteriologically-positive TB (smear- or culture-positive) FAILURE: Patient started on re-treatment regimen after failing previous treatment DEFAULT: A patient who returns to treatment, bacteriologically-positive, following a treatment interruption of two-months or more.
Determining the Case Definition Bacteriology History of TB Site of Disease Smear-negative NO New Pulmonary TB CASES Smear-positive Return after default Extra-pulmonary YES Relapse Failure Severity of Disease
Progress towards 70% case detection 80 WHO target 70% 70 60 accelerated progress: 50 target 2005 40 Cases notified under DOTS (%) 30 DOTS begins average rate of 1991 20 progress: target 2013 10 0 1990 1995 2000 2005 2010 2015 WHO, 2000
2003 Case Detection and Treatment Success Rates (WHO) 100 Malta Target zone Cambodia Cuba Tonga Maldives Viet Nam Solomon Is Peru Tunisia 90 Fiji Jamaica Bosnia & Hezegovina Hong Kong Samoa Oman Qatar Treatment success (%) Uruguay Mongolia Marshall Is Nicaragua Chile Kyrgyzstan Morocco St Lucia Kazakhstan 80 Venezuela Guatemala Djibouti Kenya El Salvador Slovenia BOTSWANA Sri Lanka French Polynesia Tanzania South Africa Turks & Caicos Is Portugal Italy Lebanon USA Latvia 70 DR Congo 80 50 60 70 90 100 110 120 DOTS detection rate (%)
Transmission of M. tuberculosis • Expelled when person with infectious TB coughs, sneezes, speaks, or sings • Spread by droplet nuclei • Close contacts at highest risk • Transmission occurs from person with infectious (active) TB disease, not latent TB infection
It’s all about VELOCITY Cough: 100 km/hr!!! Sneeze 150 km/hr!!!
TB in the Lungs Once TB bacilli is inhaled some bacilli reach the alveoli, where they are ingested by macrophages. Infection begins with the multiplication of tubercle bacilli within these alveolar macrophages. Some of the bacilli spread through the bloodstream when the macrophages die; however, the immune system response usually contains the bacilli and prevents the development of disease.
Probability TB Will Be Transmitted • Environment in which exposure occurred • Infectiousness of person with TB • Duration of exposure • Virulence of the organism
Annual Risk of Infection (ARI) • ARI is defined as a calculated average from an observed prevalence of infection, approximating the incidence of infection. • Methodology • -Sample of school-age children • -Tuberculin skin tested (Mantoux test) • Used to estimate the percentage of new TB • infections each year • Accounts for responses to non-tuberculous • mycobacterium and BCG • TST+ prevalence in Botswana in 1989 7.7% • among 6-10 y.o H. Rieder: Annual risk of infection with Mycobacterium tuberculosis. Eur Respir J 2005; 25:181-185
Pathogenesis • 10% of infected persons with normal immune systems will develop TB (lifetime risk) • HIV strongest risk factor for development of TB • - HIV infection increases the risk of developing TB disease 7% to 10% each year • In addition to HIV there are other health conditions that increase the risk of developing TB disease.
Other Conditions That Increase Risk of Progression to TB Disease • Recent infection • Substance abuse (alcohol and recreational drugs) • Diabetes mellitus • Silicosis • Malnutrition • Smoking • Some malignancies • Prolonged corticosteriod therapy • Other immunosuppressive therapy • Chest radiograph suggestive of previous TB disease
Conditions That Increase the Risk of Progression to TB Disease (cont.) • Cancer of the head and neck • Hematologic and reticuloendothelial diseases • End-stage renal disease • Intestinal bypass or gastrectomy • Chronic malabsorption syndromes • Low body weight (10% or more below the ideal)