Download
1 / 43
430 likes | 584 Views
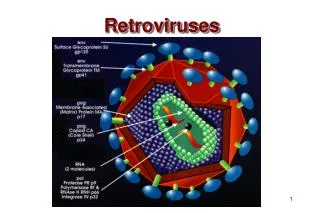
Retroviruses (chapter 38). Positive strand RNA viruses (5000-12000 bp) Enveloped Contain reverse transcriptase enzyme Copies RNA into DNA Cause chronic disease long after infection Due to integration of viral DNA into host chromosome. Number of individuals infected with HIV-1.

E N D
Retroviruses (chapter 38) • Positive strand RNA viruses (5000-12000 bp) • Enveloped • Contain reverse transcriptase enzyme • Copies RNA into DNA • Cause chronic disease long after infection • Due to integration of viral DNA into host chromosome
HIV adsorption and penetration M tropic cells of macrophage lineage Receptor/coreceptor: CD4 and CCR5 T tropic T cells Receptor/coreceptor: CD4 and CXCR4
Viral ENV protein gp120 binds to cellular receptor CD4 and to coreceptor CXCR4 or CCR5 Coreceptor interaction essential for gp41 contact and viral fusion with host cell. Small number of resistant people - lack the coreceptors Figure 65-6 Target cell binding of human immunodeficiency virus. (Redrawn from Balter M: Science 274:1988, 1996.)
HIV genome replication Part 1: synthesis of DNA Reverse transcriptase (RT) synthesizes one stand of DNA using viral RNA as the template. Reverse transcriptase (RT) synthesizes the other stand of DNA using the newly created viral single DNA strand above as the template. RT enzyme is the major target for anti-HIV drugs RT enzyme is error prone (1 error every 10000 nts!) ~1 error per genome
HIV genome replication Part 1: synthesis of DNA Cellular tRNA used as a primer by RT
HIV genome replication part 2: integration of DNA HIV genome replication part 3: transcription to create more RNA
Acquired Immune Deficiency Syndrome (AIDS) • caused by human immunodeficiency virus (HIV) • retrovirus • believed to have evolved in Africa from a monkey virus
Note initial contact is with macrophage lineage cells. Infect/stick to dendritic cells transport to lymph node - contact with CD4 T cells DTH=delayed-type hypersensitivity (Type IV hyper.) -important for controlling fungal and intracellular pathogens (bacterial and viral) DTH is mediated by CD4 T cells Neurological symptoms basis is not well understood possibly due to viral infection of neurons Possibly release of substances by other cells that promote inflammation in brain Figure 65-8 Pathogenesis of human immunodeficiency virus (HIV). HIV causes lytic and latent infection of CD4 T cells and persistent infection of cells of the monocyte macrophage family and disrupts neurons. The outcomes of these actions are immunodeficiency and acquired immune deficiency syndrome (AIDS) dementia. DTH, Delayed-type hypersensitivity. (Redrawn from Fauci AS: Science 239:617-622, 1988.)
Time-course reflects CD4 T cell numbers and the amount of virus in the blood Figure 65-9 Time course and stages of human immunodeficiency virus (HIV) disease. A long clinical latency period follows the initial mononucleosis-like symptoms. The progressive decrease in the number of CD4 T cells, even during the latency period, allows opportunistic infections to occur. The stages in HIV disease are defined by the CD4 T-cell levels and occurrence of opportunistic diseases. ARC, acquired immune deficiency syndrome (AIDS)-related complex. (Redrawn from Redfield RR, Buske DS: Sci Am 259:90-98, 1988, updated 1996.)
Importance of CD4 T cells in the initiation of an immune response and in delayed-type hypersensitivity (DTH)
Transmission • direct exposure of person’s bloodstream to body fluid containing virus • groups most at risk are (descending order): • homosexual/bisexual men • intravenous drug users • heterosexuals who have intercourse with drug users, prostitutes, and bisexuals • transfusion patients and hemophiliacs • children born of infected mothers Not transmitted by casual contact (touching, etc.) (or even kissing, sneezing, bug bites, etc.)
Data for the United States There is a risk for health care workers but transmission even through needlestick is poor (less than 1% of exposures show seroconversion)
Figure 65-12 Upper estimates of cumulative global distribution of human immunodeficiency virus (HIV) infections as of the end of 2003. The estimated cumulative global total of HIV-infected adults in 2003 was approximately 46 million. Infection rates vary widely in different regions of the world. The highest rates are in sub-Saharan Africa. (Modified from AIDS Epidemic Update, Dec 2003 www.unaids.org)
Clinical manifestations • four types of pathological changes • AIDS-related complex (ARC) • AIDS • central nervous system disease • AIDS-related cancers
ARC • fever, malaise, headaches, macular rash, weight loss, lymph node enlargement, oral candidiasis, and presence of antibodies to HIV • occurs in first few months after infection; lasts 1 to 3 weeks • can develop to full-blown AIDS
AIDS • progressive destruction of CD4+ cells leads to collapse of immune system • patient susceptible to opportunistic infections
HIV pathogenesis • involves depletion of T cells, possibly by: • disruption of plasma membrane permeability • destruction by immune system cells due to presence of gp120 in membrane • syncytia formation • integration and transposition of HIV provirus • apoptosis • may cause disruption of balance between different T cell populations • may destroy or disable dendritic cells • HIV mutates rapidly, so that it evades immune system
Disease processes associated with AIDS Pneumocytis jiroveci (formerly carinii) EBV (epstein barr virus) hairy leukoplakia on the mouth
Central nervous system disease • headaches, fever, subtle cognitive changes, abnormal reflexes, and ataxia • dementia and severe sensory and motor changes observed in advanced cases • autoimmune neuropathies, cerebrovascular disease, and brain tumors are common
AIDS-related cancers • Kaposi’s sarcoma • caused by human herpesvirus 8 • carcinoma of mouth and rectum • B-cell lymphomas
Treatment • immunodiagnostic tests for HIV antibodies or antigens (ELISA used for routine screening positives followed-up with additional tests) • RT-PCR • treatment involves: • antiviral agents • nucleoside analogue reverse transcriptase (RT) inhibitors (e.g., AZT) • nonnucleoside RT inhibitors (e.g., delavirdine) • protease inhibitors (e.g., indinavir) • Fusion-penetration inhibitors (target gp41) • treatment of opportunistic infections and cancer
Prevention and control • screening and treatment of blood and blood products • education • protected sexual behaviors • search for vaccine is ongoing
Rapid evolution of the neutralizing antibody response to HIV type 1 infection Douglas D. Richman, Terri Wrin, Susan J. Little, and Christos J. Petropoulos Proceedings of the National Academy of Sciences U S A. 2003 April 1; 100(7): 4144-4149.
Leukemia • two types of leukemias caused by retroviruses • adult T-cell leukemia • hairy-cell leukemia • HTLV-1 and -2 • Long latency period (30+ years) • both retroviruses spread: • by transfusions of contaminated blood • by needle sharing • by sexual contact • across placenta • from mother’s milk • by mosquitoes (NO)
Adult T-cell leukemia • caused by human T-cell lymphotropic virus I (HTLV-I), a retrovirus • integration of virus into host genome activates growth-promoting genes • death caused by proliferation of leukemia cells or from opportunistic infections • no treatment available
Hairy-cell leukemia • caused by HTLV-II • chronic progressive lympho-proliferative disease • death usually caused by opportunistic infections • IFN-a n3 used for treatment