Download

1 / 45
470 likes | 836 Views
Antiemetics & Related Drugs. Robert Beck, RN,BS,CCRN,SRNA Lisa Raposo , RN,BSN,CCRN,SRNA. Nausea & Vomiting. Nausea – unpleasant sensation of impending vomiting Vomiting – forceful expulsion of gastric contents through the mouth. Nausea & Vomiting. Stimuli:

E N D
Antiemetics & Related Drugs Robert Beck, RN,BS,CCRN,SRNA Lisa Raposo, RN,BSN,CCRN,SRNA
Nausea & Vomiting • Nausea – unpleasant sensation of impending vomiting • Vomiting – forceful expulsion of gastric contents through the mouth
Nausea & Vomiting • Stimuli: • Overindulgence (Food &/or Drink) • Drugs • Toxins • Inflammation/Infection • Vestibular Disorders • Pregnancy • Psychogenic Issues • Metabolic Derangements
Nausea & Vomiting • Pts report that they would rather deal with postoperative pain than N/V • Treatment Goals: • PREVENTING or relieving symptoms associated with emetogenic event • Antiemetics are MORE effective in prophylaxis than in tx • Preoperative fluid bolus to make up “deficit” • e.g. 22kg pt ~ 24⁰ maintenance fluid is 1540mL (or 64mL/⁰) • NPO for 8⁰ would be a fluid deficit of about 512mL • (100mL/kg for 1st 10kg; 50mL/kg for 2nd 10kg; 20mL/kg for remainder) • TREAT UNDERLYING CAUSE • Most episodes of acute vomiting are self limiting & require no special treatment. Treat if N/V persists. • Complications if persistent N/V left untreated: • Dehydration • Electrolyte Imbalances • Malnutrition
Epidemiology & Etiology(not all inclusive) • Drugs • ASA, NSAIDS, ETOH, opioids, antineoplastic drugs, digoxin, quinidine, erythromycin, tetracycline, nitrofurantoin, levodopa, lithium, phenytoin, theophylline, bromocriptine, hormonal therapy, Zoloft • GI • Achalasia, cholecystitis, gastric outlet obstruction, gastroparesis, gastric stasis, IBS, hepatitis, s/p surgery, incarcerated hernia, SBO, pancreatic dz, pyelonephritis, volvulus • Metabolic • Adrenal insufficiency, DKA, electrolyte imbalances, hypercalcemia, pregnancy, thyrotoxicosis, uremia, water intoxication • Neurologic • Cerebellar hemorrhage, drug withdrawal, increased ICP, migraine, head trauma, severe HTN • Psychogenic • Anorexia nervosa, physical/sexual abuse, PTSD, unpleasant sights/sounds/odors, pain, anticipatory N/V • Toxins • Staphylococcal Enterotoxin • Vestibular Disorders • Labyrinthitis, Meniere’sdz, motion sickness, benign position vertigo
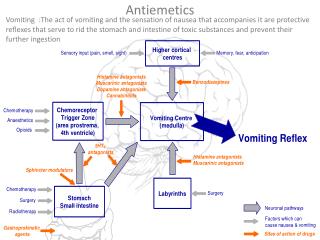
Pathophysiology • Etiologic event • (e.g. noxious substance; hypertonicity; stomach distention; drugs; vestibular disturbances; cardiac abnormalities; emotional state) • Afferent Nerve Excitation • Medullary Vomiting Center Stimulated • Glottis Closes Increased Intrapulmonic Pressure • Contractions of Respiratory Muscles • Contractions of Abdominal Muscles & Descent of Diaphragm Increased Intraabdominal Pressure • Cardiac Sphincter Relaxes Pyloric Sphincter Contracts Vomiting Occurs
Antiemetic Classifications • Antihistamines • cyclizine (Marezine); dimenhydrinate (Dramamine); diphenhydramine (Benadryl); Hydroxyzine (Vistaril/Atarax); Meclizine (Antivert/Bonine) • Serotonin Antagonists • dolasetron (Anzemet); granisetron (Kytril); ondansetron (Zofran); palonosetron (Aloxi) • Phenothiazines • chlorpromazine (Thorazine); procholorperazine (Compazine); promethazine (Phenergan); thiethylperazine (Torecan) • Prokinetic Drugs • metoclopramide (Reglan) • Cannabinoids • dronabinol (Marinol) • Miscellaneous Agent • Aprepitant (Emend); droperidol (Inapsine); trimethobenzamide (Tigan); scopolamine (TransdermScop/Transderm-V) • Benzodiazepines –(used as adjunct) • Diazepam (Valium); lorazepam (Ativan); alprazolam (Xanax) • Corticosteriods –(used as adjunct) • Dexamethasone (Decadron); Methylprednisolone (Solu-Medrol)
Antihistamines as Antiemetics • Indications • N/V associated with vestibular disturbances • Allergic rxns • Pharmacodynamics • Interrupt visceral afferent pathways • Method by which they prevent motion sickness is UNCLEAR • Pharmacokinetics • Well absorbed orally • Onset of 15-60 minutes • Peak 1-4hrs • Duration 3-8hrs • Protein binding unknown • Half lives (2-7hrs) • Biotransformation in liver; Elimination in urine • Adverse Effects • SEDATION*** • Anticholinergic: dry mouth, blurred vision, urinary retention • Paradoxical SE
Antihistamines as Antiemetics • Contraindications • Known hypersensitivity • Narrow-angle glaucoma • Premature/Newborn infants • Older adults are more sensitive to anticholinergic SE • Use CAUTIOUSLY with CV dz, thyroid dz, liver dz, pyloric obstruction, BPH • Hydroxyzine given subQ may cause tissue damage • Drug Interactions • Additive Sedation • ETOH, Antidepressants, Opioids, Sedative-Hypnotics • Enhanced Anticholinergic Effects • MAO inhibitors • Serious Cardiac Arrythmias/Prolonged QT intervals • erythromycin, clarithromycin, ketoconazole, itraconazole • Dosage Regimen • Based on specific drug & route of administration • Single doses for motion sickness (3-4x/day may be needed) & take 1-2hr before activity • See table 47-4 on page 898-99 • Lab Considerations • Allergy skin testing will be skewed when taking dramamine, benadryl, or meclizine • Discontinue dramamine 72 hrs before testing (3 days) • Discontinue Benadryl 96 hrs before testing (4 days)
Seratonin Antagonists (-setron) • Indications • PREVENTION of N/V in emetogenicantineoplastic therapies • PREVENTION of N/V in postoperative N/V • Pharmacodynamics • Seratonin (5-HT₃) receptors are located in the endings of the vagus nerve innervating the GI tract. Seratonin is released from enterochromaffin cells of GI tract, signaling seratonin receptors in the CTZ. • Antagonists BLOCK 5-HT₃ receptors in the CTZ & peripherally in the vagal and splanchnic afferent fibers from the enterochromaffin cells in the upper GI tract.
Seratonin Antagonists (-setron) • Pharmacokinetics • Rapid onset with oral/IV administration • Peak 10-60 min (drug/dose dependent) • Duration 4-24hrs (drug dependent) • Half lives (vary depending on specific drug) • Biotransformed by CYP450 enzyme (inhibitors may affect clearance); Reductions in pts with severe hepatic dz may be necessary • Adverse Effects • HA & diarrhea **MOST COMMON** • Weakness, somnolence, agitation, anxiety, and CNS stimulation • In less than 4% of pts: fever, fatigue, abnormal liver fxn, abdominal pain, HTN, pain, dizziness, chills & shivering; do not cause extrapyramidal SE as with other antiemetics because they do not block dopamine receptors • CARDIOVASCULAR: AV block, chest pain, orthostatic hypotension, myocardial ISCHEMIA, syncope, severe bradycardia, palpitations; PROLONGED QT RISK • Zofran – prolonged QT d/t blockade of K⁺ channels; Anzemet: prolonged PR/QRS/QT d/t Na⁺ channel blockade; Kytril: prolonged PR/QRS/QT Na⁺ & K⁺ channel blockade • QTc = QT ⁄ (RR)⁽⁰∙⁰⁵⁾ corrects for HR where RR = measurement from R to R in seconds (e.g. > 0.44 is prolonged is upper limit of “normal” in a pt who is NOT considered to have CV dysfunction) • Contraindications • Known hypersensitivity; Caution in Children • Pregnancy Category B (caution during pregnancy) • Use cautiously with CV disease
Seratonin Antagonists (-setron) • Drug Interactions • Serum Levels of dolasetron (Anzemet) • Increased with Cimetidine (Tagamet); Decreased with Rifampin • Decreased Clearance with Atenolol (by ¼) • Granisetron (Kytril) • Increased Risk of Extrapyramidal SE when granisetron is used with other drugs that cause such rxns • Ondansetron/Palonosetron have no significant drug interactions • -triptan drugs can be inactivated/antagonized if used with 5-HT₃ antagonists • Dosage Regimen • Dolasetron (Anzemet), Granisetron (Kytril), & Palonosetron (Aloxi) are given ONLY on days pt receives antineoplastic therapy • Ondansetron (Zofran) – 15-30 min before surgery • See table 47-4 on page 898-99 • Lab Considerations • Baseline & follow-up of LFTs • Monitor electrolytes for hypokalemia & hypomagnesemia (to reduce risk of arrhythmia-related complications)
Phenothiazines • Indications • N/V of antineoplastic therapy, toxins, radiation, motion sickness (Phenergan), intractable hiccough (Chlorpromazine) • Pharmacodynamics • Blocks dopamine receptors in CTZ • To varying degree blocks muscarininc, histamine, and norepinephrine receptors (this accounts for major adverse effects of this class) • Pharmacokinetics • Onset of 30 min-1 hr from mouth, but MORE RAPID in other routes • Peak unknown • Duration 3-12 hrs (depending on drug, dose, and route) • Most are over 90% protein bound • Chlorpromazine Half life 30 hrs • Adverse Effects & Contraindications • CNS DEPRESSION*** (Use CAUTIOUSLY in those receiving CNS depressants) • Anticholinergic: hypotension & SEDATION*** • ExtrapyramidalRxnpseudoparkinsonism, dystonia, akathisia, tardivedyskinesia; may enhance parkinsonian symptoms • Can reduce sz threshold; adjustment of antiepileptics in those with sz disorder • Pregnancy Class C
Phenothiazines • Drug Interactions • Additive Hypotension • ETOH, Nitrates • Antagonizes Oral Anticoagulants • Cardiac Arrythmias, Increased Risk of QT interval prolongation (less than some of the other medications & more with ↑dosages), CNS depression, psychomotor impairment • NUMEROUS drugs – see table 47-3 on page 897 • *potentiates action of α–blockers; levels of the drug increased with beta blocker propanolol • Dosage Regimen • Based on specific drug & route of administration; See table 47-4 on page 898-99 • Low potency – most likely to produce sedative/orthostatic hypotensive side effects • Medium potency – vary in producing sedative and extrapyramidal side effects • High potency – most likely to produce extrapyramidal effects; least likely to produce sedative or orthostatic effects • Lab Considerations • Periodic CBC & LFT – chlorpromazine (Thorazine) • Decreased H/H, leukocytes, granulocytes, and plt values • Elevated bilirubin levels, ALT, AST, and Alkaline Phosphatase values • False(+) or False(–) pregnancy tests; False(+) urine bilirubin tests • Thiethylperazine – increased prolactin levels, may interfere with gonadorelin test results
Phenothiazines BOX WARNING issued by FDA 9/16/2009 Promethazine Hydrochloride (Phenergan) “FDA is adding a BOX WARNING for PromethazineHCl (Phenergan), describing the risks of severe tissue injury, including GANGRENE, requiring amputation following venous administration . . . Perivascularextravasation, unintentional intra-arterial injection and intraneuronal or perineuronal infiltration of the drug may result in irritation and tissue damage . . . Signs and symptoms include burning or pain at site of injection, phlebitis, swelling, and blistering.” “Intravenous administration is NOT the preferred route of administration for this drug.” AACN Critical Care Newsline September 2009
Prokinetic Drug • Indications • N/V associated with lack of or depressed GI motility • Drug of choice for highly emetic antineoplastic drugs • Pharmacodynamics • Blocks DOPAMINE receptors in CTZ • Increases upper GI motility, resting tone of esophogeal sphincter, gastric contractions, & peristalsis of duodenum/jejenum by enhancing actions of acetylcholine • Pharmacokinetics • Well absorbed from GI tract, rectal mucosa, and IM tissue sites • Crosses Blood-brain barrier and placenta • Enters breast milk in greater concentrations than plasma • Onset of 1-3 minutes IV; 10-15 minutes IM; 30-60 minutes PO • Peak unknown except for IM, which is immediate • Duration 1-2 hrs • Protein binding 30% • Half lives (2.5-5 hrs) • Partial Biotransformation in liver; 25% Eliminated in urine as unchanged drug • Adverse Effects • Sedation & Diarrhea in high doses • SIGNIFICANT extrapyramidal effects (esp. in children) at high doses*** • 25% of adults 18-30 years old develop dystonia after receiving a high dose (2mg/kg/dose) • Can be prevented/controlled by giving BENADRYL***, benztropine, or diazepam
Prokinetic Drug • Contraindications • Presence of GI obstruction, hemorrhage, or perforation • Pregnancy Class B • Safe for breastfeeding infants if mother taking <45mg/day • Drug Interactions • Additive CNS Depression • ETOH, Antidepressants, Antihistamines, General Anesthetics, Opioids, Sedative-Hypnotics • Antagonization of GI effects of metoclopramide (Reglan) • Anticholinergics, Opioids • Increased Risk of HYPERTENSIVE CRISIS • MAO inhibitors • Cyclosporine Toxicity • INSULIN ADJUSTMENT in pts on insulin therapy may be required • d/t decreased absorption of food nutrients to the intestine • Increased risk of Neuromuscular Blockade (NMB) • Succinylcholine • Increased risk of EPS • haloperidol (Haldol); phenothiazines • Dosage Regimen • Varies with use; will give near end of surgery for PONV; CAUTION WITH SUCCS. • See table 47-4 on page 898-99 • Lab Considerations • LFTs may be altered • Increases in serum prolactin and aldosterone
Cannabinoids as Antiemetics • Indications • Marinol approved by FDA for antineoplastic therapy related N/V • Used ONLY after failure of other medications to prevent N/V • Use has declined since 5-HT₃ antagonists have appeared on market • Appetite stimulant to prevent/reverse wt loss for AIDS pts • Pharmacodynamics • Activates receptors in vomiting center responsible for N/V suppression • Pharmacokinetics • Use at least 6-12 hrs BEFORE antineoplastic therapy; Onset unknown • Peak 2 hrs • Duration 4 hrs • Highly lipid soluble; enters breast milk in HIGH concentrations • Half lives (25-36 hrs) • Biotransformed extensively with 10-20% bioavailability
Cannabinoids as Antiemetics • Adverse Effects • Dysphoria, detachment, depersonalization, & temporal deterioration • Younger pts tolerate better than older. • USE CAUTIOUSLY WITH CV dz • Tachycardia, hypotension, & CNS effects • Contraindications • Known hypersensitivity to Marinol, marijuana, or SESAME OIL • Do not use in N/V r/t other causes • Lactating Mothers • Safety in children under 18 has not been established • Drug Interactions • Additive CNS depression • ETOH, Antihistamines, Tricyclic Antidepressants, Opioids, Sedative-Hypnotics • Increased Tachycardia Risks • Amphetamines, cocaine, sympathomimetics, anticholinergics, antihistamines, and tricyclic antidepressants • Dosage Regimen • Twice daily
Misc. Drugs in Antiemetic Therapy • Droperidol (Inapsine) – blocks dopamine receptors in CTZ • Similar SE as phenothiazines (esp. EPS, sedation, hypotension) • ***CONTRAINDICATED for: hypersensitivity, narrow-angle glaucoma, bone marrow supression, CNS depression, severe liver/cardiac dz, known intolerance, and children <2 yrs old • Trimethobenzamide (Tigan) – unclassified antiemetic; dopamine blockade • Mild-moderate N/V; can be given IM • Injection site pain, but other adverse effects are rare • INCREASED RISK of Reye’s Syndrome in children with viral illnesses • Lethal in Liver/Brain, but affects all organs; www.reyessyndrome.org • Scopolamine (TransdermScop) – anticholinergic (muscarinic antagonist) • Prophylaxis/treatment of motion sickness by reducing vestibular hyperstimulation • May dilate pupil on same side as patch; Anticholinergic SE • Benzodiazepines (e.g. Diazepam, Lorazepam) – Anxiolytic • Anticipatory N/V • N/V prevention/control through anxiolysis • Corticosteroids (e.g. Dexamethasone, Methylprednisolone) • Proven adjuvent in N/V therapy as “add on”
Test Question 1 A 48 year old patient presents with N/V that has persisted for 2 days. He is currently not under the care of a physician for any other health issues or taking any medications (Rx or OTC). He has NKDA/NKFA. You have received the following information from the nurse: • Glucose: 90 K⁺: 2.9 Mg: 1.1 • EKG shows: P wave: 0.20 QRS: 0.12 QTc: 0.54 HR: 125 • PVCs are present intermittently Based on the information given, which of the following antiemetic medications is most appropriate for you as the practitioner order for this pt at this time? • dronabinol (Marinol) po • ondansetron (Zofran) iv • promethazine (Phenergan) pr • hydroxyzine (Atarax/Vistaril) subQ
Aprepitant (Emend) • Aprepitant (Emend) – Neurokinin₁ (NK₁) antagonist • Selectively antagonizes Substance P and NK₁ receptors to reduce N/V • Inhibits CYP 3A4 enzyme & could potentially elevate plasma concentrations of interacting drugs (antineoplastics) • Not recommended for chronic N/V prevention
Single-dose aprepitantvsondansetron for the prevention of postoperative nausea and vomiting . • ARTICLE INFO: • Study comprised of 42 centers • 8 U.S. sites and 34 non-U.S. sitesin North America, South America, Europe, Australia, and Asia • randomized double-blind study (Protocol091) • Approval fromthe Institutional Review Board for each center was obtainedand all patients gave written informed consent. • Pts selected for this study were undergoing general anesthesia for abdominal surgery British Journal of Anaesthesia, 2007
Single-dose aprepitantvsondansetron for the prevention of postoperative nausea and vomiting . . . • BACKGROUND: • Aprepitant- neurokinin antagonist (effective for chemo induced N/V prophylaxis) • Compared Aprepitant with Zofran for prevention of post-op N/V • METHODS: • 982 pts receiving Anesthesia for major abd surgery • Pts receive either PO Aprepitant 40mg, PO Aprepitant 125mg, or IV Zofran 4mg pre-op • randomized, double-blind trial • N/V and use of rescue therapy were documented for 48hr post op
Single-dose aprepitantvsondansetron for the prevention of postoperative nausea and vomiting . . . • FINDINGS: • Aprepitant at both doses superior to Zofran for COMPLETE response 0-24hr post-op • Aprepitant was superior to Zofran for NO VOMITING 0-24hr • Aprepitant was superior to Zofran for NO VOMITING 0-48hr • Distribution of peak nausea scores were lower in both Aprepitant groups vs. Zofran
Single-dose aprepitantvsondansetron for the prevention of postoperative nausea and vomiting . . . • CONCLUSION: • Aprepitant significantly more effective the Zofran for prevention of vomiting post op at both 24 and 48hr post op, and in decreasing nausea severity in 1st 48hr after surgery. • Aprepitant was generally well tolerated • ***Additional literature shows that Aprepitant has no effect on prolonged QTc interval in patients receiving therapy.
MECLIZINE IN COMBINATION WITH ZOFRAN FOR PREVENTION OF POSTOPERATIVE NAUSEA AND VOMITING IN HIGH-RISK POPULATION AANA 2007
MECLIZINE IN COMBINATION WITH ZOFRAN FOR PREVENTION OF POSTOPERATIVE NAUSEA AND VOMITING IN HIGH-RISK POPULATION • PURPOSE: • Compare use of a multimodal approach combining Meclizine and Zofran with a unimodal approach using a placebo and Zofran for prevention of PONV in a high-risk population
MECLIZINE IN COMBINATION WITH ZOFRAN FOR PREVENTION OF POSTOPERATIVE NAUSEA AND VOMITING IN HIGH-RISK POPULATION • Materials & Methods: • Randomized, double blind, parallel groups, institutional review board approved study • Randomized 77 individuals • 84 subjects enrolled, 7 were removed r/t breaches in protocol or changes in anesthetic management = 77 pts • Screened for 4 of 5 PONV for experimental or control group assignment • PONV high risk group: (incidence: 17% no factors present, 87% with all 5 present) • General anesthesia (incidence is 20-30% in population, therefore higher institutional and pt costs, and decreased pt satisfaction) • Female • Non-smoker • Motion sickness • PONV history
MECLIZINE IN COMBINATION WITH ZOFRAN FOR PREVENTION OF POSTOPERATIVE NAUSEA AND VOMITING IN HIGH-RISK POPULATION • Materials & Methods (cont): • INCLUSION: • Pts consented for surgery with general anesthesia scheduled for 60min or longer • ASA classification I or II • Ages 18-65 • English language proficiency • Presence of 4 of 5 risk factors • EXCLUSION: • Contraindications for receiving general anesthesia • Hx of sensitivity to Zofran or Meclizine • Antiemetic use within 24hr of surgery • Pregnancy • GERD • Obesity with BMI >35% • No significant differences in demographics (excluding weight), surgical or anesthesia time, or nausea incidence in the PACU
MECLIZINE IN COMBINATION WITH ZOFRAN FOR PREVENTION OF POSTOPERATIVE NAUSEA AND VOMITING IN HIGH-RISK POPULATION • Materials & Methods (cont): • Meclizine (x2- 25mg = 50mg) or Placebo given to pt prior to procedure • inexpensive, high duration of effectiveness, few side effects • Zofran (4mg) given to pt 15-30 prior to end of procedure (admin to both groups) • highly effective, very expensive • Emergency antiemetics: Zofran, Reglan, Phenergan
MECLIZINE IN COMBINATION WITH ZOFRAN FOR PREVENTION OF POSTOPERATIVE NAUSEA AND VOMITING IN HIGH-RISK POPULATION • Materials & Methods (cont): • Severity of PONV was rated on a 0-10 verbal numeric rating scale (VNRS) • Measured variables • Time to onset • Incidence of PONV • Total antiemetic requirements
MECLIZINE IN COMBINATION WITH ZOFRAN FOR PREVENTION OF POSTOPERATIVE NAUSEA AND VOMITING IN HIGH-RISK POPULATION • RESULTS: • With the exception of weight, there was no significant differences in relation to demographic variability, surgical time, anesthetic time, smoking history, history of motion sickness, or PONV • No exception of amount of anesthetic agent or narcotics administered between groups • Incidence of vomiting similar between groups at all interval measurements both in the hospital and at home • Meclizine group had lower VNRS scores at 15 and 45 minutes following rescue treatment • Incidence of nausea was lower in the Meclizine vs. placebo group (10% vs. 29%) • Prophylactic Meclizine resulted in lower incidence of severity of PONV in high risk population
MECLIZINE IN COMBINATION WITH ZOFRAN FOR PREVENTION OF POSTOPERATIVE NAUSEA AND VOMITING IN HIGH-RISK POPULATION • CONCLUSION: • Administration of Meclizine in combination with Zofran for prevention of PONV in high-risk population had significant effects during post-op period in the hospital and home environment • PONV persists as a common complaint following general anesthesia, in part because a remarkable growth of outpt surgery and emphasis on mobilization and discharge • Due to managing PONV being challenging and costly, pts in high-risk population must be identified accurately pre-operatively
MECLIZINE IN COMBINATION WITH ZOFRAN FOR PREVENTION OF POSTOPERATIVE NAUSEA AND VOMITING IN HIGH-RISK POPULATION • CONCLUSION (cont): • Based upon study- the low cost, minimal side effect profile, and efficiency of PONV prevention may make Meclizine an ideal agent to administer in combination with Zofran to prevent PONV • Combo of pre-op Meclizine and intra-op Zofran improved subjects response in emergency antiemetics, allowed for longer nausea free-period post operatively, decreased nausea incidence post discharge compared with placebo and Zofran • FISHER EXACT TEST POWER ANALYSIS: • Incidence of nausea 74% with 4 risk factors • Decreased to approximately 35% with use of Zofran • Decreased further to 10% with combination of Zofran and Meclizine • Study suggests that combination antiemetic therapy is more effective than monotherapy, especially for those in the high-risk group
Test Question 1 A 48 year old patient presents with N/V that has persisted for 2 days. He is currently not under the care of a physician for any other health issues or taking any medications (Rx or OTC). He has NKDA/NKFA. You have received the following information from the nurse: • Glucose: 90 K⁺: 2.9 Mg: 1.1 • EKG shows: P wave: 0.20 QRS: 0.12 QT: 0.54 HR: 125 • PVCs are present intermittently Based on the information given, which of the following antiemetic medications is most appropriate for you as the practitioner order for this pt at this time? • dronabinol (Marinol) po • ondansetron (Zofran) iv • promethazine (Phenergan) pr • hydroxyzine (Atarax/Vistaril) subQ
Test Question 1 A 48 year old patient presents with N/V that has persisted for 2 days. He is currently not under the care of a physician for any other health issues or taking any medications (Rx or OTC). He has NKDA/NKFA. You have received the following information from the nurse: • Glucose: 90 K⁺: 2.9 Mg: 1.1 • EKG shows: P wave: 0.20 QRS: 0.12 QT: 0.54 HR: 125 • PVCs are present intermittently Based on the information given, which of the following antiemetic medications is most appropriate for you as the practitioner order for this pt at this time? • dronabinol (Marinol) po • cannabinoids are not appropriate for this pt as an antiemetic; po route for an actively vomiting pt is not an appropriate route • ondansetron (Zofran) iv • d/t the prolonged QT interval, hypomagnesemia, & hypokalemia, Seratonin Antagonists are NOT appropriate for this patient • promethazine (Phenergan) pr • PR is an appropriate route; promethazine (in this case) is the most appropriate drug to be given • hydroxyzine (Atarax/Vistaril) subQ • this medication given subQ can cause tissue damage
Test Question 2 A relatively new antiemetic approved by the FDA has been shown to be very effective in decreasing postoperative N/V, as well as N/V elicited after antineoplastic therapy. It has also been noted to have no associated QTcelongation that has been shown with other antiemetic therapy. What is the name of this drug? • dronabinol (Marinol) • dolasetron (Anzemet) • sertraline (Zoloft) • aprepitant (Emend)
Test Question 2 A relatively new antiemetic approved by the FDA has been shown to be very effective in decreasing postoperative N/V, as well as N/V elicited after antineoplastic therapy. It has also been noted to have no associated QTcelongation shown with other antiemetic therapy. What is the name of this drug? • dronabinol (Marinol) • No. Dronabinol is only used in antineoplastic therapy as a last-line agent or as an appetite stimulant in AIDS pts. • dolasetron (Anzemet) • No. The Serotonin Antagonists have been shown to prolong QTc intervals. • sertraline (Zoloft) • No. Zoloft has been shown to CAUSE N/V in pts • aprepitant (Emend) • Yes. Aprepitant (Emend) is a newly approved drug from the FDA that has shown significant improvements in PONV and N/V in pts receiving antineoplastic therapy. There is also no QTc elongation noted with its use.
Test Question 3 Antiemetic combination therapy has NOT been shown to be effective in the control of PONV or N/V associated with antineoplastic therapy. True/False
Test Question 3 Antiemetic combination therapy has NOT been shown to be effective in the control of PONV or N/V associated with antineoplastic therapy. False • Research has shown combination therapy to be very effective, cost-effective, and increases pt satisfaction when used appropriately.
References Diemunsch, P., et al. (2007). Single-dose aprepitantvsondansetron for the prevention of postoperative nausea and vomiting. British Journal of Anaesthesia, 01-10. Forrester, C.M. (2007). Meclizine in combination with zofran for prevention of postoperative nausea and vomiting in high-risk population. AANA, 75(1), 27-33. Gutierrez K (2008). Antiemetics & Related Drugs. Pharmacotherapeutics. St. Louis: Saunders. Jacnicki, P.K. (2009). Effect of 5 HT3-Receptor Antagonists on QTc Interval Prolongation in Patients with Common NOS1AP Variant. The Internet Journal of Anesthesiology, 20(1), Retrieved from http://www.ispub.com/journal/the_internet_journal_of_anesthesiology/volume_20_number_1/article/effect_of_5_ht3_receptor_antagonists_on_qtc_interval_prolongation_in_patients_with_common_nos1ap_variant.html Marbury, T.C. (2009). Lack of effect of aprepitant or its prodrugfosaprepitant on QTc intervals in healthy subjects. Anesthesia & Analgesia, 109(418-425), Retrieved from http://www.anesthesia-analgesia.org/cgi/content/abstract/109/2/418