Download
1 / 34
1.07k likes | 8.08k Views
CASE PRESENTATION ON TIBIAL FRACTURE. PREPARED BY REMYA VISHWAMBARAN EMERGENCY ROOM. DEMOGRAPHIC DATA. NAME : MR.S.K.R AGE/SEX : 40YRS/MALE

E N D
CASE PRESENTATION ON TIBIAL FRACTURE PREPARED BY REMYA VISHWAMBARAN EMERGENCY ROOM
DEMOGRAPHIC DATA • NAME : MR.S.K.R • AGE/SEX : 40YRS/MALE • IP NO : 196279 • DATE OF ADMISSION : 09/02/13 • COMPLAINTS : MULTIPLE LACERATED WOUNDS IN RT LEG,PAIN IN RT WRIST,TENDERNESS OVER LT KNEE • DIAGNOSIS : COMMINUTED TIBIAL SHAFT FRACTURE • DISCHARGED ON :30/12/12
PHYSICAL ASSESMENT GENERAL APPEARANCE • Patient was drowsy for several minutes • Unable to mobilize his rt lower extremity. VITAL SIGNS OF THE PATIENT ARE BP : 120/80 mm of hg PR :86/mt RR :16/mt SPO2 : 98%
SKIN • Skin is warm to touch. • Tenderness over rt ankle • Laceration on rt toes • Noted abrasions on rt lower limb. • HEADAND NECK • Hair Is Equally Disrtibuted. • Absence Of Dandruff. EYES • Ableto move both eyes
EARS • Patients pinna is same color as facial. • Able to hear sounds clearly . • No discharges • NECK AND THROAT • Lips are pink but dry. • Teeth is properly aligned with no dentures. • No tenderness of node. THORAX The Thorax Is Symmetric On Inspection
CARDIO VASCULAR • Absence Of Chest Pain • Heart sounds are clear. • Upon auscultation his Bp is 120/80mmof hg. GENITO URINARY • Normal pubic hair GASTRO INTESTINAL • No Tender Ness Of Abdomen and its soft .
MUSCULOSKELETAL • Unable To Mobilize His Lt Lower Limb. • Has Pain During Examination. • Tenderness at site of fracture • Lower extremity appear shortened NEUROLOGIC • To Follow Commands. • No neurovascular deficit.
Patient History • PRESENT MEDICAL HISTORY Patient was brought to E.R by REDCRESCENT ambulance after he was involved in R.T.A with complaints of : • MULTIPLE LACERATED WOUNDS IN Rt LEG,PAIN IN RT WRIST,TENDERNESS OVER LT KNEE. Patient was diagnosed with comminuted fracture on tibial shaft rt leg. • PRESENTSURGICAL HISTORY • He underwent external fixation of tibia on the same day of admission as an emergency case • PAST MEDICAL AND SURGICAL HISTORY No past history
Investigations Done For The Patient 1.X-Ray skull ,chest ,hand and ankle 2. CT Scan (lumbosacralspine,lower extremity) 3.Blood investigations like • PT INR • SERUM ELECTROLYTES • RH TYPING and ABO • CBC
TREATMENT DONE FOR THE PATIENT • SURGICAL INTERVENTION_ EXTERNAL FIXATION OF RT TIBIA. • Medications IV FLUIDS • N.S 0.9% Dextrose 5% ANTIBIOTICS • inj . augmentin 1.2 gm iv tid • inj. flagyl 500mg iv bd • inj .amikacin 500mg iv bd • ANALGESICS • diclofenac 75mg im . • pethedine 50 mg im.
Tibial shaft fracture • The tibia is the larger bone in your lower leg. Tibial shaft fractures occur along the length of the bone.
Types of Tibial Shaft Fractures The tibia can break in several ways. The severity of the fracture usually depends on the amount of force that caused the break. The fibula is often broken as well. Common types of tibial fractures include • Stable fracture:This type of fracture is barely out of place. The broken ends of the bones basically line up correctly and are aligned. In a stable fracture, the bones usually stay in place during healing. • Displaced fracture: When a bone breaks and is displaced, the broken ends are separated and do not line up. These types of fractures often require surgery to put the pieces back together.
Transverse fracture: • This type of fracture has a horizontal fracture line. This fracture can be unstable, especially if the fibula is also broken. • Oblique fracture: • This type of fracture has an angled pattern and is typically unstable. If an oblique fracture is initially stable or minimally displaced, over time it can become more out of place. This is especially true if the fibula is not broken.
Spiral fracture: • This type of fracture is caused by a twisting force. The result is a spiral-shaped fracture line about the bone, like a staircase. Spiral fractures can be displaced or stable, depending on how much force causes the fracture. • Comminuted fracture: • This type of fracture is very unstable. The bone shatters into three or more pieces. • Open fracture: • When broken bones break through the skin, they are called open or compound fractures. • Open fractures often involve much more damage to the surrounding muscles, tendons, and ligaments. They have a higher risk for complications and take a longer time to heal. • Closed fracture: • With this injury, the broken bones do not break the skin. • Although the skin is not broken, internal soft tissues can still be badly damaged. • In extreme cases, excessive swelling may cut off blood supply and lead to muscle death, and in rare cases, amputation.
ANATOMYAND PHYSIOLOGY Tibia is medial bone of the leg, also known as shinbone or shankbone. It is larger and stronger of the two bones of leg, i.e. it is stronger and longer than fibula.It connects the knee with ankle and is the major weight bearing force of body.Like all other typical long bones, it has two ends and an intervening shaft. The cross-section of tibia is triangular in shape
Proximal end of tibia: • The proximal end of tibia is expanded and is a bearing surface for weight of the body, which is transmitted through femur. • There are massive medial and lateral condyles and an intercondylar area intervening between the condyles. There is also a prominent tibialtuberosity • Condyles: • There are two condyles of tibia: medial and lateral. • Both condyles have an articular surface proximally, which articulates with corresponding condyles of femur. • There is an intercondylararea between the two condyles, which marks the separation between the two. Both condyles are visible and palpable in living subjects.Lateral condyle has a fibular facet for attachment of fibula. • ii. TibialTuberosity: • Is a little projection in the area where the anterior condylar surface merge with each other. • It is divided into a proximal smooth and a distal rough region. To the smooth part of tibialtuberosity attaches the patellar tendon.
B.Shaft of tibia: • shaft of tibia is triangular in cross section. Consequently, it consists of three borders and three surfaces. • Borders: • The borders of tibia are named as: anterior border, medial border and lateral (interosseous border). • Surfaces: • The surfaces of tibial shaft are named as: anteromedial surface, posterior surface and lateral surface • C .Distal end of Tibia: • Distal end is slightly expanded and has 5 surfaces namely anterior, medial, posterior, lateral and distal • The distal end of tibia is rotated laterally, an effect known as tibial torsion. • The lateral surface of distal end contains the triangular fibular notch for attachemnt of fibula. • Medial Malleolus: • It is a strong pyramidal process prolonged from the distal end of the tibia medially.It ends proximal to the lateral malleolus, which is also more posterior. Its main role is to deepen the articular surface for ankle joint.
Tibia/Fibula - Anterior view • Lateral tibial plateau • Tibialtuberosity • Fibular head • Fibular shaft • Lateral malleolus • Tibia plafond • Medial malleolus • Tibia shaft • 9.Medial tibial plateau
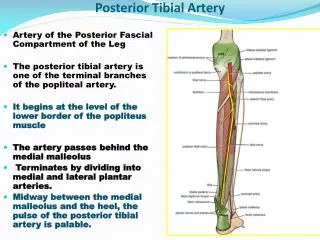
BLOOD SUPPLY TO TIBIA Proximal end receives its blood supply form metaphyseal vessels, which arise from genicular arterial anastomosis.Nutrient foramen of tibia usually lies near the soleal line. The nutrient artery which is transmitted through this foramen comes from posterior tibial artery. • The periosteal blood supply to the shaft arises from anterior tibial artery. • metaphysis receives its blood from anastomosis around the ankle joint.
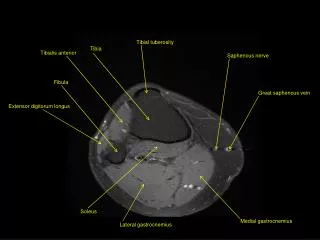
The muscles of the leg may be divided into three groups: anterior, posterior, and lateral. The Anterior Crural Muscles Tibialis anterior.Extensor digitorumlongus. Extensor hallucislongus.Peronæustertius The Posterior Crural Muscles—The muscles of the back of the leg are subdivided two groups—superficial and deep. The Deep Group TheSuperficialGroup Gastrocnemius. Soleus. Plantaris Popliteus. Flexor hallucislongus. flexor digitoriuslongus ,tibialis posterior
ETIOLOGY • High-energy collisions, such as an automobile or motorcycle crash. • Sports injuries, such as a fall while skiing or running into another player during soccer. SIGNS AND SYMPTOMS • Pain. • Inability to walk or bear weight on the leg. • Deformity or instability of the leg. • Bone "tenting" the skin or protruding through a break in the skin. • Occasional loss of feeling in the foot. • Obvious deformity such as angulation or shortening (the legs are not the same length) • Breaks in the skin • Contusions (bruises) • Swelling • Bony prominences under the skin • Instability (some patients may retain a degree of stability if the fibula remains intact or the fracture is incomplete)
. Treatment Nonsurgical Treatment Nonsurgical treatment may be recommended for patients who: • Are poor surgical candidates due to their overall health problems • Are less active, so are better able to tolerate small degrees of angulation or differences in leg length • Have closed fractures with only two major bone fragments and little displacement • Initial treatment. • Your doctor may initially apply a splint to provide comfort and support. Unlike a full cast, a splint can be tightened or loosened, and allows swelling to occur safely. • Cast and functional brace. • One proven nonsurgical treatment method is to immobilize the fracture in a cast for initial healing. After weeks in the cast, it can be replaced with a functional brace made of plastic and fasteners. The brace will provide protection and support until healing is complete.
Surgical Treatment • Intramedullary Nailing. The current most popular form of surgical treatment for tibial fractures is imnailing. • Plates and screws These tools are reserved for fractures in which intramedullary nailing may not be possible or optimal, such as certain fractures that extend into either the knee or ankle joints. • External fixation. In this type of operation, metal pins or screws are placed into the bone above and below the fracture site.
Complications • Sharp fragments may cut or tear adjacent muscles, nerves, or blood vessels. • Excessive swelling may lead to compartment syndrome, a condition in which the swelling cuts off blood supply to the leg. This can result in severe consequences and requires emergency surgery once it is diagnosed. • Open fractures can result in long-term deep bony infection or osteomyelitis, although prevention of infection has improved dramatically over the past generation. Surgical Complications • Malalignment, or the inability to correctly position the broken fragments • Infection • Nerve injury • Vascular injury Blood clots (these may also occur without surgery) • Nonunion (failure of bone to heal) • Angulation (with treatment by external fixation
NURSING INTERVENTIONS 1.Provide emergency care if requires (hemostasis, respiratory care, prevention of shock).2. Provide fracture fixation to prevent following injury of tissues.3. Monitor fluids input and output continuously, insert IV catheter, urinary catheter. 4. Monitor client’s vital signs. provide care to a client with cast (observe signs of circulatory impairment – change in skin color and temperature, diminished distal pulses, pain and swelling of the extremity;) 5.Monitor client’s laboratory tests results for abnormal values.6. Administer IV therapanalgesics,antibiotics, and other medications as prescribed.7. Prepare client and his family for surgical intervention if required 8.Observe for signs of thrombophlebitis, report immediately.9. Provide appropriate skin care to prevent pressure sores.10. Encourage fluid intake and high-protein, high-vitamin, high-calcium diet.11. Teach the client appropriate crutch-walking techniques . 12.Provide emotional support to client, explain all procedures to decrease anxiety and to obtain cooperation.13. Instruct client regarding fracture healing process, diagnostic procedures, treatment and its complications.
PRIORITIZATIONOF NURSING PROBLEMS • Acute Pain Related To Fracture • Impaired Physical Mobility Secondary To Fracture • Knowledge Deficit Regarding Treatment Regimen And Disease Condition. • Risk For Infection Due To open fracture. • .
NURSING HEALTH TEACHING • Encourage early ambulation by using crutches and wheel chair. • Encourage him to perform passive and active excercises. • Discuss prevention of recurrent fractures. • Teach symptoms needing attention such as numbness,decreasedfunction,increasedpain,elevated temperature. • Teach the importance of follow up care. • Encourage follow up medical supervision to monitor for union problems. • Encourage adequate balanced diet to promote bone and soft tissue healing.
conclusion • A CASE OF RTA PATIENT WITH FRACTURE OF TIBIAL SHAFT WAS UNABLE TO MOVE HIS LEFT LOWER EXTREMITY. • PATIENT HAD UNDERGONE EXTERNAL FIXATION OF TIBIA AND D FIBULA ON SAME DAY OF ADMISSION (09/02/13) AS AN INITIAL EMERGENCY CARE AND LATER HE HAD UNDERGONE IM NAILING OF TIBIA • PATIENT WAS DISCHARGED ON 24/02/13 • PATIENT WAS INSTRUCTED FOR FOLLOW-UP AFTER 2 WEEKS.
Bibiliography • .Lippincott manual of nursing practices 9 th edition. • www.sports injury .advice .com • Grays anatomy and physiology • Wikipedia