Download

1 / 27
270 likes | 446 Views
Geert M. Verleden Medical Director Lung Transplant Programme Leuven, Belgium. WHO and WHEN TO REFER FOR LUNG TRANSPLANTATION?. Patient selection : indications for LTx. Patients with chronic end-stage lung disease , such as COPD, CF, PAH, Pulmonary fibrosis Max 50-55 y for HLTx

E N D
Geert M. Verleden Medical Director Lung Transplant Programme Leuven, Belgium WHO and WHEN TO REFER FOR LUNG TRANSPLANTATION?
Patientselection: indicationsforLTx • Patientswithchronicend-stagelungdisease, such as COPD, CF, PAH, Pulmonaryfibrosis • Max 50-55 y forHLTx • 60-65 y forLTx • Failingmedicaltreatment • Ornomedicaltreatmentexists • Needfor • Information • Demonstration of adequate healthbehavior • Willingness to adhere to guidelines Aim of LTx: survival benefit and increase in QOL
Meaning of failingmedicaltreatment? • COPD • Rehabilitation • LVRS?? • Bullectomy • IPF and ILD • Studyprotocols? • CF • WhataboutmulitiresistentPseudomonasorCepacia?
Regarding PAH • Need expertise in treatmentwith • Prostaglandins • PDE inhibitors • Endothelin receptor blockers • …
Absolute contra-indications • Malignancy in the last 2 years, exceptcutaneoussquamous and basalcell tumors • Remainsquestionnableregardingforinstancebreastcancer, renalcancer. How long tumor free? • Untreatableadvanceddysfunction of otherorgans (kidney, liver, …) • Unlesscombinedtransplantation • Untreatablecoronaryarterydisease • What is nowadaysuntreatable? • Non-curablechronicextrapulmonaryinfections (hep B, hep C, HIV) • Alsoquestionnable
Absolute contra-indications • Significant chestwall/spinaldeformity • To bediscussedwithsurgeons • Documentednon-adherence • Specificproblem in young CF patients • Untreatablepsychiatricorpsychologicconditionwithinability to complywithmedicaltherapy • Absence of social support • Difficulties to adhere to strictfollow up protocols • Substanceaddiction: tobacco, alcohol, narcotics, drug abusethat is activeorwithin the last 6 months • Is sixmonthsenoughdelay?
Relativecontra-indications • Age > 60-65 y • Criticalorunstableclinicalcondition (invasiveventilation, ECMO)
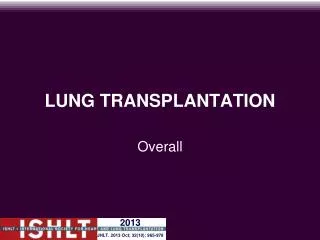
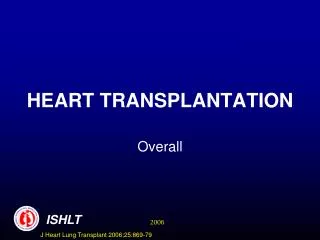
Risk Factors for 1 Year Mortality (N=11,079) J Heart Lung Transplant 2008;27: 937-983
Risk Factors for 1 Year MortalityRecipient Age J Heart Lung Transplant 2008;27: 937-983
Risk Factors for 5 Year MortalityRecipient Age J Heart Lung Transplant 2008;27: 937-983
Risk Factors for 1 Year MortalityCenter Volume J Heart Lung Transplant 2008;27: 937-983
Relativecontra-indications • Colonizationwithhighlyresistantor virulent bacteria, fungi ormycobacteria • CF patientsspecifically • Mycobacterialcolonization/infectionremainsproblematic
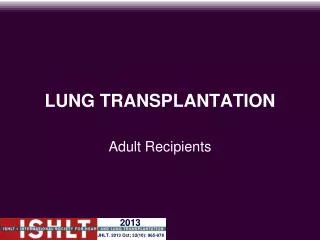
ADULT LUNG TRANSPLANTATIONSurvival By Diagnosis CF vs. COPD: p < 0.0001 CF vs. IPF: p < 0.0001 CF vs. PPH: p < 0.0001 CF vs. Sarcoidosis: p < 0.0001 J Heart Lung Transplant 2008;27: 937-983
Relativecontra-indications • BMI > 30 • Severeorsymptomaticosteoporosis • Diabetes • arterialhypertension • peptic ulcer • GER (50% or more preTx) • … ShouldbeadequatelytreatedbeforeTx
When to refer? • Disease-specific criteria: • Orens et al. International guidelinesfor the selection of lung transplant candidates: 2006 update--a consensus report from the PulmonaryScientificCouncil of the International Society forHeart and LungTransplantation. J HeartLung Transplant 2006; 25: 745. • Takinginto account severalcentrecharacteristics: • Donor availability • Localwaiting time
Increasingrole of DCD donors N=17 N=126
Time windowreferral - transplantation Referral Transplantation < expected survival before Tx Waiting time If estimated WT > expected survival Decline for Tx ? Urgent Tx ?
Waiting time is bloodgroupdependent Days Blood Group P<0.001
300 200 100 0 …and heigthdependent days p < 0.05 219 167 (175 ± 6 cm) (160 ± 7 cm) > 168 cm < 168 cm Adaptedfrom D. Van Raemdonck, Leuven 2003
How to refer: role of the Tx Team Transplantation protocol Describing procedures, localresponsabilities, treatmentmodalities, … Collaborationwith other MD disciplines Director(s) of the program Pulmonologist Surgeon Other MD Establisha Networkwith Referring physicians Collaborationwith paramedics, such as Nurses, physiotherapists, Dieticians, socialworkers, Psychologist, … Collaborationwith Transplant coordinators
How to refer? • Telephone call • Withreferringphysician • To discusscurrentpatientsituation • First outpatientvisit • To see the patientpersonally and to givefurherinformationonwhat to expect • Ifnoclearcontra-indicationssofar • Pretransplantwork-upperformedbyreferringphysician • Afterwards team discussion and short admission to the transplant hospital • Onwaiting list Promoteearlyreferral !!
Conclusions • General indications and contra-indications provide guidelinesforTx • Specificdisease-based criteria willbehelpfull • No single criteria is enough to predict prognosis • Best option: • Contact transplant center and discuss the patient • Refer the patientfor a first “physical” contact whenin doubt Be on time !!! Do not let the referringphysiciandecide to transplant ornot