Download
1 / 32
320 likes | 326 Views
This study explores how social connectedness mediates the relationship between chronic pain and suicide ideation, focusing on its impact on psychological processes and emotional reactions. The presentation discusses the prevalence of chronic pain, how pain becomes chronic, and the psychological aspects influencing pain perception and coping strategies. It also delves into the behavioral reactions associated with chronic pain, emphasizing the importance of understanding and addressing social aspects to mitigate suicide risk.

E N D
Chronic Pain and Suicide Ideation: The Mediating Effect of Social Connectedness. Margaret Legarreta, PhD1,3,; Erin McGlade, PhD1,2,3; Deborah Yurgelun-Todd, PhD1,2,3 Salt Lake City, Rocky Mountain, VISN 19 Mental Illness, Research, Education and Clinical Center (MIRECC)1; University of Utah, School of Medicine, Department of Psychiatry2 Cognitive Neuroimaging Laboratory3
Disclaimer This presentation is based on work supported, in part, by the Department of Veterans Affairs, but does not necessarily represent the views of the Department of Veterans Affairs or the United States Government. None of the authors listed have conflicts to report. This project is supported by the Military Suicide Research Consortium (MSRC), an effort supported by the Office of the Assistant Secretary of Defense for Health Affairs under Award No. W81XWH-10-2-0178 Conflicts Statement of Funding
Overview Study Goal/Question: Can the relationship between pain and suicide be explained by social connectedness? Chronic Pain Suicide Behaviors Social Connectedness Current Study Discussion
Why Social Connectedness Conducted Pain Groups in VA 29 y/o Male Low back pain, radiated to his feet Low frustration tolerance and was isolating from his family – autistic son who compounded his inability to function in the family His progress…
Chronic Pain Pain – experience that is unpleasant & associated with actual or potential tissue damage1 Temporary Related to a stimulus Chronic Pain – extends months to many years2 No longer a reliable indicator of damage2,3 Less efficient alarm system 3 Typically distinguished from acute pain based on temporal characteristics • Typical duration – 3 to 6 months 3,4 Mersky & Bogduk, 19941; Garland, 20122; Lumely et al., 20013; Bonezzi, Demartini, & Buonocore, 20124
Prevalence of Chronic Pain Common phenomenon impacting more that 116 million Americans1 One sixth to ¼ of adults report significant persistent pain1,2. One quarter of adolescents also report chronic pain3,4. Persistent pain is more prevalent among Veterans5. 47% report mild pain 28% report moderate to severe 75% total pain reporting Bonezzi et al.,1; Ilgen, Zivin, McCammon, & Valenstein, 20082; van Tilburg et al., 20113; Reigstad, Jorgensen, & Wichstrom, 20064; Spelman et al., 20125
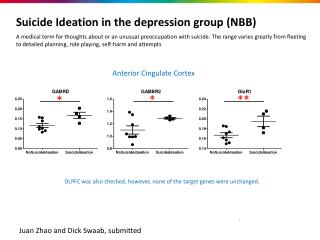
How Pain become Chronic Imagining and the Pain Matrix Matrix includes: primary & secondary somatosensory cortex, insula, anterior cingulate cortex, amygdala, prefrontal cortex & thalamus.1 Most regions are thought to perform sensory discriminations However, anterior cingulate cortex isbelieved to process the affective components of pain1,2 The brain is thought to change over time in response to persistent pain. Henry, Chiodo, & Yang, 20111; Garland, 20122; Apkarian et al., 20043
How Pain becomes Chronic Central Sensitization Maintains and exacerbates pain through changes in the brain1. Brain and spinal cord are active in generating persistent pain through reductions in pain threshold1,2. • Changes result in: amplified pain response, pain to a previously non-painful stimulus, and/or increased duration of the perception of stimulus presence1,3,4. • Can also result in spontaneous pain2,3,4. Lumley et al., 20111; Latremoliere & Woolf, 20092; Bonezzi et al., 20123; Curatolo, Arendt-Nielsen, & Petersen-Felix, 20064
Psychological Aspects of Chronic Pain Reciprocal Relationship: Pain Psychological processes. Attention Important in processing of pain signals1,2 • More focus on painful stimuli results will likely result in great pain intensity • Distraction from pain can result in less pain intensity. Cognition/Thinking Interpretation of pain also impacts perceptions of pain intensity1 • If pain is thought of as sensory information not necessarily linked to tissue damage, pain is perceived as less intense and individual experience less functional impairment1,3,4. • If a person perceives they have some control over their pain, or they can cope with the pain, the pain will be perceived as less intense. • Pain catastrophizing has been linked to more physical impairment & disability and greater psychological distress to include risk of suicide5,6,7. Garland, 20121; Henry et al., 20112; Chung et al., 20123; Gatchel et al., 20074; Cheatle. 20115; Edwards et al., 20066; Legarreta et al., 20177
Psychological Aspects of Chronic Pain Emotional Reactions Pain often leads to negative emotions such as fear, anger, and sadness1,2. These emotional responses can trigger autonomic processes such as stress related muscle construction which can become a self-perpetuating cycle2,3,4. Behavioral Reactions – Social aspects of chronic pain1 A reduction in activity typically occurs in the presence of pain Long-tern activity reduction, or even kinesiophobia serve to increase pain and disability related to pain Avoidant behaviors are reinforced • Reduction of potential future injury • Family and friends may experience reduced expectations Garland, 20121; Gatchel, 20072; Ilgen et al., 20083; Edwards, Smith, & Haythornthwaite, 20064;
Suicide Behaviors Self-injurious behavior carried out with the intent to end one’s own life1,2 Encompasses a wide range of – death by suicide to a self-aborted attempt1,2 Suicide Attempt – any behavior that can kill an individual and the person involved has some level of intent to die1,2 Exists along a spectrum Suicide Ideation – thinking of suicide without acting upon the thoughts1,2 Graded levels of risk Risk increases as an individual has devised more specific plans Nock et al., 20081; Mann, 20022
Prevalence of Suicide In 2009 suicide was 10th leading cause of death for individuals 10 years of age or greater1,2. Research has suggested that rates of suicide in Veteran populations may be double the rates of those in civilian populations3. Braden & Sullivan, 20081; Cheatle, 20112; Kaplan et al., 20073
Risk Factors for Suicide Braden & Sullivan, 20081; Nock et al., 20082; Gaynes et al., 20043; Mann, 20024; Van Orden et al., 20105
Chronic Pain & Suicide Chronic pain is associated with increased risk of suicide1. Suicide ideation is 2-3 times greater in individuals with chronic pain2. Death by suicide is 2x greater individuals with persistent pain1. 17-66% of people with chronic pain report serious thoughts of suicide1,3,4,5. 20% of people with pain report a suicide attempt in their lifetime3. Cheatle, 20111; Edwards et al., 20062; Ilgen et al., 20083; Fishbain et al., 20124; Smith et al., 20045
Pain Factors associated with Suicide Risk Cheatle, 20111; Braden & Sullivan, 20082; Fishbain., 20123; Ilgen et al., 20084
Social Connectedness How people come together and interact. Quality and number of connections one has with others. 6 Components to determine quality connections Duration of relationship Frequency of interaction with the other person Knowledge of the connection’s goals Intimacy or closeness with the person Self-disclosure with the person Familiarity with the person’s social circle Aron et al., 1991
Social Connectedness & Pain Chronic pain - a process that resets interpersonal parameters, creating separation from the world and other people1. Patients report restricted freedom, and a feeling of being imprisoned1,2. Chronic pain patients report needing to keep their condition secrete2. They believe people will think negatively about them once their condition is know. Relationships often exacerbate the chronic pain condition1,3 Cyclical pattern where more is done for the patient, thereby reducing their activity, and increasing the pain experienced. Patient may become dependent upon their partner or children Increased care of the patient creates strained relationship Thomas, 20001; Snelling, 19942; Smith, 20033
Social Connectedness & Suicide Much work has been done here under different terms Social disconnection Thwarted Belonging1 Factors of disconnection related to mortality Living alone, loss of a spouse, loneliness interpersonal discord & low social support2,3,4,5 Increased social connection has been shown to reduce risk for suicide6 Further, the sense of “pulling together” has been shown to have a preventive effect7. Joiner, 20051; Waern, Runeson, & Allebeck, 20052; Conwell, Rotenberg, & Caine, 19903; Rubenowitz et al., 20114; Turvey et al., 20025; Hoyer & Lund, 19936; Joiner, Hollar, & Van Orden, 20077; Trout, 19808
Study Design Participants 80 male and female Veterans from the Salt Lake Community Assessment Cross-sectional • McGill Pain Inventory (McGill) • Columbia Suicide Severity Rating Scale (CSSRS) • Social Connectedness Scale Completed in one study visit of approximately 90 minutes
Participants Basic Demographics
Measures Social Connectedness – 5 Item Scale Cronbach’s Alpha = .931 Each item scored 0 (not at all like me) to 7 (very true for me). Range is 5 - 35 Columbia Suicide Severity Rating Scale (CSSRS) Interview based suicide measure that assess differing levels of SI and SA. McGill Pain Questionnaire Self-Report Inventory • Select a varied of words that describe your pain. Words scores are totaled and a score is provided Range of 0 - 80
Results Suicide Descriptions
Results Pain Descriptions
Results: Mediation Analysis We investigated whether social connectedness (M) mediates the relationship between chronic pain (X) and suicidal ideation (Y) in veterans using the PROCESS procedure in SPSS. Social Connectedness Path b t=-3.7,p=0.0005 Coefficient=-0.102 CI: -0.16,-0.046 Path a t=-2.29,p=0.02 Coefficient=-0.15 CI: -0.28,-0.197 Path c t=2.8,p=0.007 Coefficient=0.044 CI: 0.012,0.075 Suicidal Ideation Chronic Pain Path c’ t=1.94, p=0.0564 Coefficient=0.028 CI: -0.0008, 0.0573
Results: Continued • Chronic Pain correlates (X) with Social Connectedness (M) (path a) • Social Connectedness (M) correlates with Suicidal Ideation (Y) after controlling for Chronic Pain (X) (path b) • Chronic Pain (X) correlates with Suicidal Ideation (Y) (Path c) • Chronic Pain does not correlate with Suicidal Ideation (Y) after controlling for Social Connectedness (M) (Path c’) (CI does not include 0). Thus, Social Connectedness statistically mediates the relationship between Chronic Pain and Suicidal Ideation. • Social Connectedness mediates less than half of the total effect of Chronic Pain on Suicidal Ideation (ratio of indirect to total effect=0.355). Thus, there is evidence of partial mediation.
Conclusions Chronic Pain was related to SI – higher pain intensity was related more active SI. Chronic Pain was related to social connectedness – higher pain intensity was related less social connectedness. SI was related to social connectedness – as level of SI increased, reported social connection decreased. Social connectedness help partially explain the connection between chronic pain and SI.
Discussion Reduce suicide by reducing comorbid pain & increasing social connectedness? Research that reduced pain reduces suicide? Increased connection reduces suicide • Family connection, events and being a fan1,2 • Other mediators? Insomnia and Catastrophizing 3,4 Current Treatment for Suicide Treating conditions associated with suicide (ie depression, ptsd, etc.) Treating acute suicide crisis – attempts or SI with specific plans (hospitalization) Treatment specifically targeting suicide behaviors • Only 40-60 randomized trial currently5 • 1/3 of trials showed positive effect, and only 2 replicated • DBT – decreases SBs by up to 50% during treatment • Caring Letters – send letters at intervals to those who do not attend follow-up referral appointments. • Many more being tested currently! ; Hoyer & Lund, 19931; Joiner, Hollar, & Van Orden, 20072; Cheatle, 20113; Legarreta et al., 20164; Ward-Ciesielski, Tidik, Edwards, & Linehan, 20175
Discussion Current Treatment for Pain CBT for Chronic pain ACT for chronic pain VA has very strong pain management programs • Pittsburgh • Minneapolis • Tampa Social Connectedness in Veterans Limited understanding currently Multiple time points of interest • Pre-Military, during deployment, between deployment, and post deployment Henry, Chiodo, & Yang, 20111; Garland, 20122; Apkarian et al., 20043
Military Culture – Fit with unit 8 of 80 Participants reported not fitting in • “17 going on 12, I didn’t fit in.” • “I was generally a loner, I didn’t fit in, didn’t chase women, party, drink, or smoke.” • “I never quite fit in anywhere, but I wasn’t an outcast either.” Many reported moderate fit with their unit • “I fit in fairly well.” • “Fine” • “In active duty I was ok, it was better in the reserves.” Many report fitting in well • “My unit was tight. I fit right in with all my peers and leaders.” • “Fit in real well. Great camaraderie. Superior efforts of action.” • “My unit were my bothers and it was one of the happiest times of my life.” • “I loved the Army. I feel I fit in and performed well.”
Future Directions Understand Social connectedness in Veterans more fully Examine the differing intervals in veterans lives to understand connectedness across time Understanding the interplay between pain, suicide behaviors, Examine SI and SA both Examine change in SBs when social connectedness and/or chronic pain is altered
Hypothesis and Data Analytic Plan The relationship between chronic pain and suicide will be mediated by difference in social connectedness. Data Analysis – Mediation Analysis Mediation hypotheses posit how, or by what means an independent variable (X) affects an outcome variable (Y) through potential intervening variables or mediators (M) Fig A: X affects Y (path c, total effect) Fig B: Simple mediation model showing how variable X’s effect on Y can be apportioned into an indirect effect via M and a direct effect on Y Path a: Effect of X on M Path b: Effect of M on Y controlling for X Indirect effect: a*b Path c: Effect of X on Y (total effect) Path c’: Effect of X on Y controlling for M (direct effect) The total effect of X on Y can be expressed as a sum of the direct and indirect effects: c=c’+ab Baron & Kenny, 19861; Preacher & Hayes, 20082