Download
1 / 17
210 likes | 2k Views
Guillian-Barre Syndrome. Dr. Belal M. Hijji, RN. PhD December 7 & 10, 2011. Learning Outcomes. At the end of this lecture, students will be able to: Describe the pathophysiology, clinical manifestations, and medical management of Guillain-Barré syndrome.

E N D
Guillian-Barre Syndrome Dr. Belal M. Hijji, RN. PhD December 7 & 10, 2011
Learning Outcomes At the end of this lecture, students will be able to: • Describe the pathophysiology, clinical manifestations, and medical management of Guillain-Barré syndrome. • Use the nursing process as a framework for care of patients with Guillain-Barré syndrome.
Introduction • Guillain-Barré syndrome is an autoimmune attack of the peripheral nerve myelin. The result is acute, rapid segmental demyelination of peripheral nerves and some cranial nerves, producing ascending weakness with dyskinesia (inability to execute voluntary movements), hyporeflexia (subnormal or absent reflexes), and paresthesias (numbness). • Myelin is a complex substance that covers nerves, providing insulation and speeding the conduction of impulses from the cell body to the dendrites. It is produced by Schwann cells that are spared, allowing for remyelination in the recovery phase of the disease
Antecedent Events • A respiratory or gastrointestinal infection, although vaccination, pregnancy, and surgery were identifed as antecedents. Infection with Campylobacter jejuni (a relatively common gastrointestinal bacterial pathogen) precedes Guillain-Barreé syndrome in a few cases. • The antecedent event usually occurs 2 weeks before symptoms begin. Weakness usually begins in the legs and progresses upward for about 1 month.
Pathophysiology • Guillain-Barré is the result of a cell-mediated immune attack on peripheral nerve myelin proteins. The best-accepted theory is that an infectious organism contains an amino acid that mimics the peripheral nerve myelin protein. The immune system cannot distinguish between the two proteins and attacks nerve myelin causing inflammation and destruction and the axon is left unable to support nerve conduction.
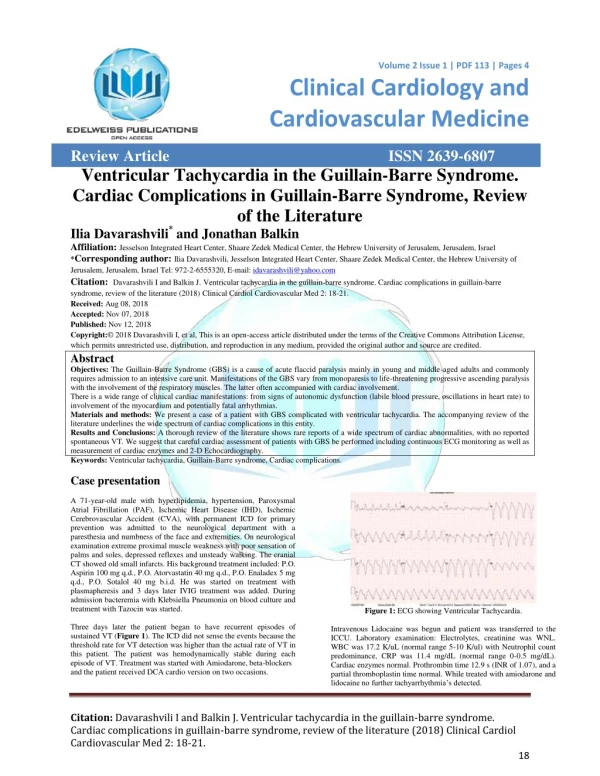
Clinical Manifestations • Initially muscle weakness and diminished reflexes of the lower extremities. • Neuromuscular respiratory failure. • Sensory symptoms include paresthesias of the hands and feet and pain related to the demyelination of sensory fibers. • Optic nerve demyelination may result in blindness. • Bulbar muscle weakness related to demyelination of the glossopharyngeal and vagus nerves results in an inability to swallow or clear secretions. Vagus nerve demyelination results in autonomic dysfunction, manifested by instability of the cardiovascular system. Patients may have tachycardia, bradycardia, hypertension, or orthostatic hypotension. These problems occur and resolve rapidly.
Assessment and Diagnostic Findings • Symmetric weakness, hyporeflexia, and upward progression of motor weakness. • A history of a viral illness is suggestive of the diagnosis. • Changes in 2 respiratory function tests, which are the vital capacity and negative inspiratory force (< 25 cm H2O) are assessed to identify impending neuromuscular respiratory failure. Vital capacity is the maximum amount of air a person can expel from the lungs after a maximum inspiration. • Serum laboratory tests are not useful in the diagnosis. • Elevated protein levels are detected in CSF evaluation.
Medical Management • This syndrome presents a medical emergency in view of rapid progression and neuromuscular respiratory failure, requiring ICU admission. • Mechanical ventilation may be necessary to support pulmonary function and adequate oxygenation, and may be required for an extended period. • Weaning from mechanical ventilation occurs when the respiratory muscles can again support spontaneous respiration and maintain adequate tissue oxygenation.
Anticoagulant agents and thigh-high elastic compression stockings or sequential compression are used to prevent complications. • Plasmapheresis and intravenous immunoglobulin (IVIG) are used to directly affect the peripheral nerve myelin antibody level. Both therapies decrease circulating antibody levels and reduce the amount of time the patient is immobilized and dependent on mechanical ventilation. • The cardiovascular risks of tachycardia and hypertension are treated with alpha-adrenergic blocking agents (Doxazosin, Prazosin, Terazosin, Tamsulosin, Alfuzosin). Hypotension is managed by increasing the amount of IV fluid administered.
Nursing Management of Patient WithGuillain-Barre Syndrome • Assessment • Ongoing assessment for disease progression is critical. The patient is monitored for life-threatening complications (respiratory failure, cardiac dysrhythmias, DVTs) so that appropriate interventions can be initiated. • Nursing diagnoses • Ineffective breathing pattern and impaired gas exchange related to rapidly progressive weakness and impending respiratory failure. • Impaired physical mobility related to paralysis.
Planning and goals • Improved respiratory function • Increased mobility • Nursing interventions (maintaining respiratory function) • Use of incentive spirometry and chest physiotherapy. • Monitoring for changes in vital capacity and negative inspiratory force are key to early intervention for respiratory failure. • Mechanical ventilation is required if the vital capacity falls, making spontaneous breathing impossible and tissue oxygenation inadequate.
Indications for initiating mechanical ventilation include a vital capacity of 12 to 15 mL/kg, downward vital capacity trend over 4 to 6 hours, and an inability to clear secretions. • Discussion of the potential need for mechanical ventilation should be carried out with the patient and family on admission. • Intubation and mechanical ventilation will result in less anxiety if it is initiated on a nonemergent basis to a well-informed patient. • Suctioning may be needed to maintain a clear airway. • The nurse assesses the blood pressure and heart rate frequently. • Medications are administered or a temporary pacemaker is placed for clinically significant bradycardia.
Nursing interventions (Enhancing physical mobility and preventing complications) • Supporting paralysed extremities in functional positions (The splint held the hand in the functional resting position: wrist positioned between 10° and 30° extension, thumb in opposition and abduction, and semiflexion of the finger joints (Fig. 1), and passive range-of-motion exercises are performed at least twice daily.
Nursing interventions (Enhancing physical mobility and preventing complications) (Continued….) • Performing range-of-motion exercises, altering positioning, anticoagulation, thigh-high elastic compression stockings or sequential compression boots, and adequate hydration. • Padding may be placed over bony prominences such as the elbows and heels. • Evaluating laboratory test results that may indicate malnutrition or dehydration. • Collaboration with the physician and dietitian to meet the patient’s nutritional and hydration needs.
Evaluation (Expected patient outcomes). The patient: • Maintains effective respirations and airway clearance • Has normal breath sounds on auscultation • Demonstrates gradual improvement in respiratory function • Shows increasing mobility • Regains use of extremities • Participates in rehabilitation program • Demonstrates no contractures and minimal muscle atrophy