Download
1 / 77
910 likes | 1.72k Views
Devital extirpation, amputation and combined method of pulpitis treatment. Mummification, stages complication. Comparative characteristics of different methods of pulpitis treatment. Cleaning and Shaping of the Root Canal System. Objectives of Canal Preparation. Start with the end in mind.

E N D
Devital extirpation, amputation and combined method of pulpitis treatment. Mummification, stages complication. Comparative characteristics of different methods of pulpitis treatment.
Objectives of Canal Preparation Start with the end in mind
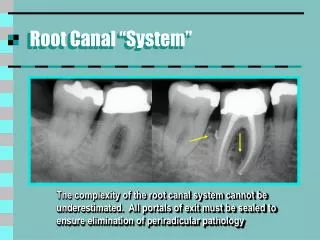
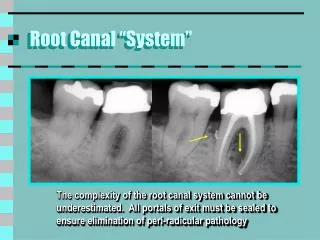
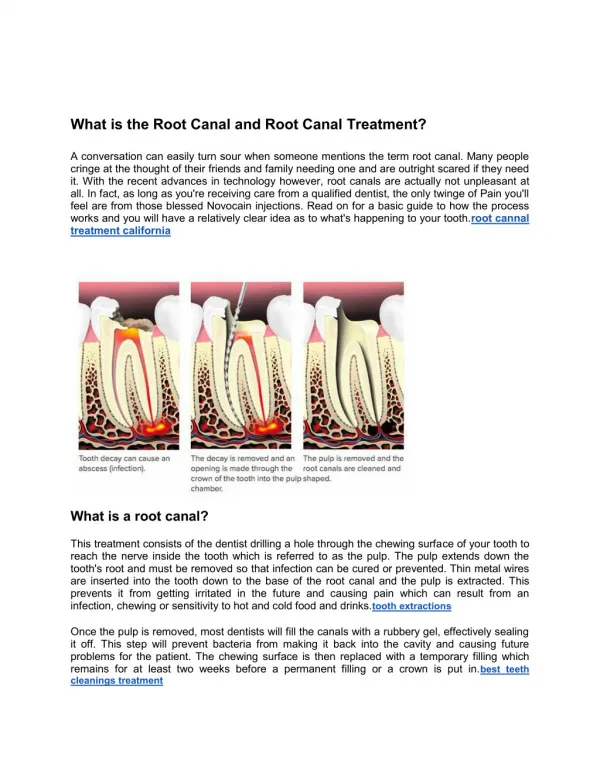
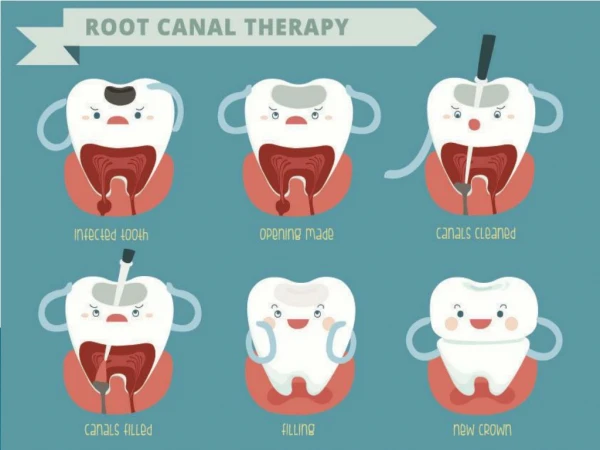
Objectives of root canal preparation The root canal system must be: • Cleaned of its organic remnants • Shaped to receive a three dimensional filling of the entire root canal space
Objectives of root canal preparation The canal is • First cleansed by irrigation • Then shaped by instrumentation
Cleansing of the root canal Objectives • Removal of organic debris • Elimination of bacteria
Irrigation An ideal irrigant: • Is nontoxic • Dissolves vital and necrotic tissue • Is bactericidal • Lubricates the canal • Removes the smear layer
Sodium hypochlorite • Dissolves vital and necrotic tissue • Is bactericidal • Lubricates the canal
Prolube EDTA and carbamide peroxide in a water soluble base
Prolube • Facilitates placement of file • Entraps debris • Helps in removal of the smear layer
EDTA • Chelating agent • Effectively removes smear layer
Shaping of the root canal • Canal shape – produced by instrumentation • Objective is a smooth tapered preparation
Instruments Instruments differ according to: • Metal • Taper • Tip design • Cross sectional geometry • Length of cutting blades • Sizing
Nickel titanium Stainless steel Excellent flexibility Less flexible Conforms to canal Straightens and curvature transports canal Plastic deformation Permanent deformation Metals
Metals Stainless steel files demonstrate permanent deformation
Metals Nickel titanium files demonstrate plastic deformation
Taper Definition Increase in diameter per unit length
0.32 mm diameter increase D16 D1 What is Taper? D16 D1 0.96 mm diameter increase
Tip Design • Non-cutting tip • Bullet nose (60 degree) tip • Smooth transition angle where tip meets flat radial lands
Tip Design • Designed to follow a pilot hole • Guides instrument through canal during preparation
Cross-sectional geometry • Three radial lands • Each contains bidirectional cutting edges • Keep instrument centered in the canal • Cutting edges scrape dentin
Cross sectional geometry • Radial lands separated by three u-shaped flutes • Provide space for accumulation of debris • Moves debris out of canal
Length of cutting blade • Traditionally 16 mm • Orifice shapers – 10 mm
Sizing of instruments ISO sizes • Number refers to tip diameter in tenths of mm • The tip diameter increases by 0.05 mm from sizes 10 to 60, then by 0.10 mm
Sizing of instruments • % increase in diameter from #10 to #15 file is 50% • Difference between #55 and #60 is only 9%
Sizing of instruments Series 29 • Progressive 29% increase in tip diameter • Instruments are better spaced • More instruments in smaller sizes and fewer large instruments
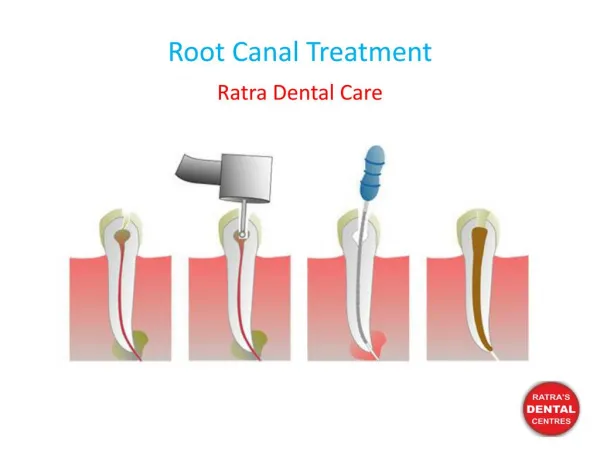
Crown Down Technique • The coronal portion is prepared before the apical portion • Follows medical principle of cleansing before probing a wound
Crown Down Technique • Eliminates constrictions in the coronal region • Reduces effect of canal curvature • Improves tactile awareness during apical preparation
Crown Down Technique • Allows more effective irrigation • Removes majority of tissue and microbes before apical third is approached • Reduces change in working length during apical preparation
Crown Down Technique • Coronal third Orifice shapers • Middle third 0.06 taper rotary Profiles • Apical third 0.04 taper hand Profiles
Clinical Procedure • Estimate working length • Parallel radiograph • Estimated working length is the distance from the reference point to the radiographic apex
Clinical Procedure • Establish straight line access to apical third
Clinical Procedure Explore the canal • Ensure that canal corresponds to radiographic apex • Small file – #10 K-file • May need to precurve these SS files
Clinical Procedure • Files used in a push/pull or quarter turn pull motion • Never rotate these files through 360 degrees
Clinical Procedure Estimate canal size • Radiographic appearance • Crown/root morphology • Standardized tables
Estimation of canal size See Table in manual
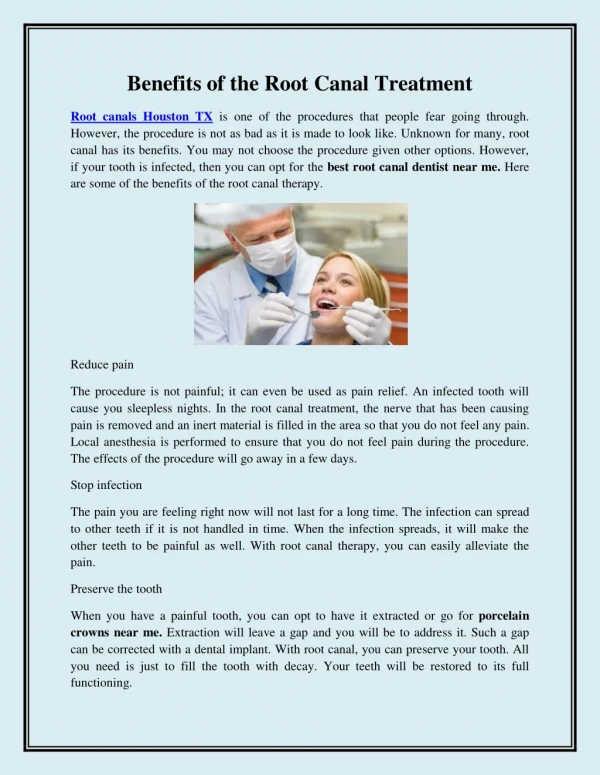
Clinical Procedure Actual Working Length determination Preparation should terminate at • Apical constriction • 1 mm short of radiographic apex
Clinical Technique Actual Working Length determination • Radiograph • Apex locator
Clinical Procedure Actual Working Length Determination