Download
1 / 35
350 likes | 374 Views
Study on total hip replacement in sickle cell patients <40 years, analyzing complications, anatomical abnormalities, risk factors, and outcomes.

E N D
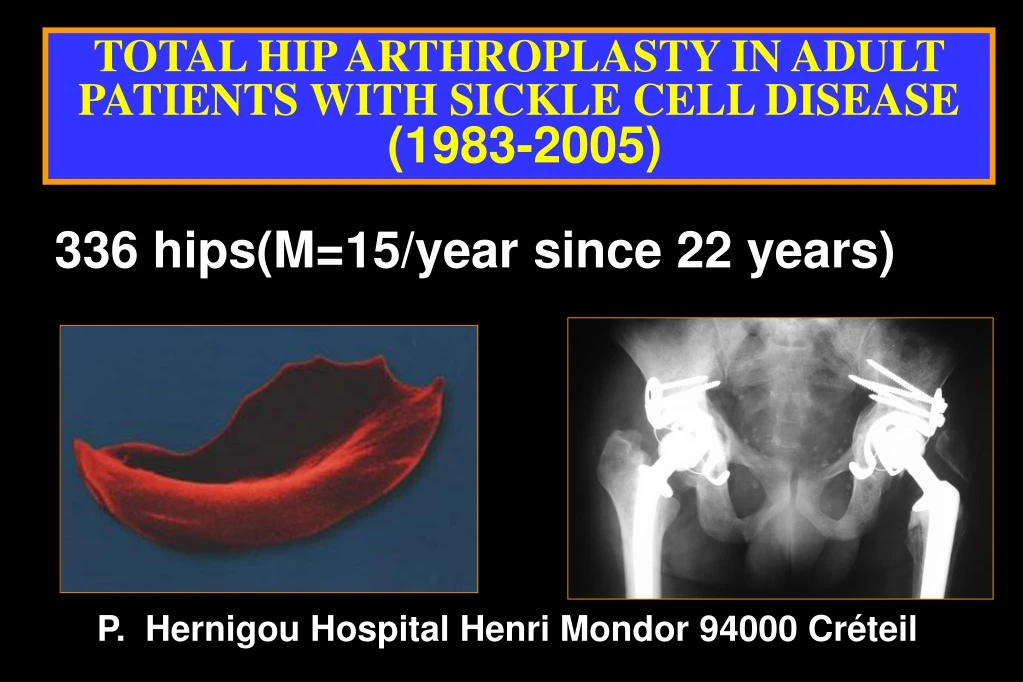
TOTAL HIP ARTHROPLASTY IN ADULT PATIENTS WITH SICKLE CELL DISEASE(1983-2005) P. Hernigou Hospital Henri Mondor 94000 Créteil 336 hips(M=15/year since 22 years)
SICKLE CELL DISEASE Total hip replacement in such patients who are less than forty years old has been associated with high rates of complications and revisions. Also, the majority of such patients with sickle cell disease have been reported to have a high prevalence of failure of components fixation The purpose of the present study was to analyze the results after primary total hip arthroplasty with cement in a group of patients who had sickle cell disease
Problems • anatomic abnormalities • infection of the hip during childhood • Transfusions and anemia • Allo immunisation • Pulmonary Infarctus • Revisions
The anatomic abnormalities • The anatomic abnormalities may include • abnormal location of neurovascular structures secondary to soft-tissue contractures, • an abnormal location of the hip center, • a limb-length discrepancy, • a small acetabulum and femoral canal • increased anteversion of the proximal part of the femur.
Levels of Deformity Femoral Neck Deformity Greater Trochanteric Deformity
Levels of Deformity Metaphyseal Deformityas a result of an osteotomy.
OSTEOTOMIES 20 ans
Problems • anatomic abnormalities • infection of the hip during childhood • Transfusions and anemia • Allo immunisation • Pulmonary Infarctus • Revisions
10 hips in patients who had had infection of the hip during childhood All the hips had cemented total hip replacements. The age of the patients at the time that the infection was contracted was an average of 12 years). The average age of the patients at the time of the total hip arthroplasty was 32.4 years. The interval between active infection and arthroplasty was 24 years. All the hips had a quiescent period of infection of more than ten years. The average duration of follow-up was 8 years (range, five to fifteen years). Two hips had recurrence of infection.
Fémur anormal inégalité
Problems • anatomic abnormalities • infection of the hip during childhood • Transfusions and anemia • Allo immunisation • Pulmonary Infarctus • Revisions
Problems • anatomic abnormalities • infection of the hip during childhood • Transfusions and anemia • Allo immunisation • Pulmonary Infarctus • Revisions
Results:336 hips average follow-up: 10 years(10 to 20) 60 THA >10 years
336 protheses Revisions: 6 % 22 revisions Infections 3 1 revision 7 2 revisions 2 3 revisions 1 4 revisions 3
Conclusion • The management of hip arthroplasty with sickle cell disease requires recognition of anatomical deformities • Assessment begins in the preoperative period with recognition of significant risk factors, including previous surgery systemic medical conditions, as well as selection of suitable components.