Download
1 / 22
220 likes | 513 Views
NICU 3/2010 Skills Day Education Compiled by, June Amling RN, MSN Pamela Allen RN Pam Dozier RN, BSN. NICU Basics for Tracheostomy Care. The “ Musts ” for Tracheostomy Patients. Signs, Guidelines, & ‘Ready to

E N D
NICU 3/2010 Skills Day Education Compiled by, June Amling RN, MSN Pamela Allen RN Pam Dozier RN, BSN NICU Basics for Tracheostomy Care
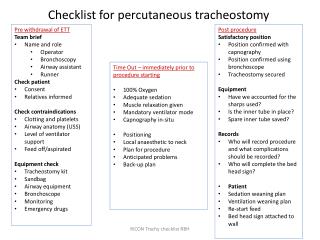
The “Musts” for Tracheostomy Patients Signs, Guidelines, & ‘Ready to Go Bag’ Hyperextension & Off-loading • Copy of the NPG (found under Nursing Policies on the Intranet) • ‘Critical Airway Sign’ for fresh post-op trach patient. • “I have a Tracheostomy”signat bedside & must be kept updated • Respiratory card on the ventilator with tracheostomy specifications • ‘Ready to Go’ Bag • Keep the yellow/green label on the front package of a customized Bivonatracheostomy box. The cover lists the specific re-ordering info for that patient’s trach. Tuck this in the patient’s “Ready to Go” bag.
Important Points to Remember with the Fresh Post-op Tracheostomy Patient *Keep patient’s head midline & hyperextendedat all times. *Trach care must be done with cluster cares ie: q3-4hrs. * Assess stoma site with each cluster cares. Look for any skin breakdown around neck or at stoma site. *Ties are not to be changed until after the first trach change has been done by ENT (usually 5-7days post-op) *‘For preventative reasons & upon returning from OR apply 2 pieces of Replicare Thin’ inferior & superior to trach stoma. Replace as needed. * Do not cut the stay sutures that are secured to the chest. Add additional Tegaderm if the tape appears loose. *Notify ENT if you feel at any time the trach ties are too tight or loose during the first week. It is not uncommon for swelling post-op which may create tightness with ties. Call ENT! *Take care with ventilator tubing minimizing tension to stoma site & that it s not directly resting on patient’s skin. See photo to right.
‘Ready-to-Go’ BagIncludes the Following Items & must be checked by RN at the beginning of the shift. Same Size Tracheostomy tube 2. One size smaller tracheostomy, or an appropriate ETT Next size smaller than a 3.0ped/neo is a 2.5 ETT or 8 fr suction catheter 3. 8 Fr Suction Catheter (for emergency decannulation) 4. Surgilube 5. Suture Removal Kit 6. Velcro ties
CRITICAL AIRWAY Fresh Post-Op Tracheostomy 1. The first week is very crucial in preserving the integrity of the stoma, therefore you must keep the patient’s head midline & hyperextendedat all times. You must do a thorough assessment to occipital area for pressure ulcers with routine cares Q 3-4 hours. Do not place infant on the full body size Z-Flo mattress , but it is acceptable to use the small 7 X 7 inch Z-Flo directly under the head. When using the Z-Flo, continue to maintain midline positioning & hyperextension with the use of a neck roll. 2. Please be very diligent with trach care. Trach care must be done with cluster cares (ie: q 3-4 hours). Spray the tips of the ‘Qtips with wound cleanser and clean around the stoma and underneath the trach ties. Assess superior & inferior aspects of stoma site with each cluster care as to be certain trach is not applying too much pressure to skin. Document assessment in Powerchart (Ongoing Assessment→Tracheostomy →Stoma site). 3. Make certain that intact Replicare Thin pieces are superior & inferior to the trach stoma at all times. If Replicare becomes soiled, or loose, be sure to change Replicare Thin to areas previously stated, as well as underneath the stay sutures. Avoid additional tension to the stay sutures by carefully applying Replicare Thin underneath stay sutures. Notify ENT if you feel at any time the trach ties are too tight or loose during the first week. 4. After ENT performs the first trach change, ties are to be changed qd & prnif moist. If copious secretions are present change Replicare Thin & ties BID. Be certain to assess and cleanse back of neck during trach cares. 5. A small air leak is acceptable if the patient is ventilating satisfactory. If not, please notify ENT. 6. Must have Ready-to –Go bag at bedside, a tracheostomy sign with a copy of the CNMCTracheostomy Nursing Practice Guideline within easy reach. _____________ *If you have any questions regarding trach care, please contact June Amling pg #0183, Pam Allen pg #4676 &/or any other team member of the NICU Skin/Wound Care committee. List of member names are posted in the team room on the leadership board.
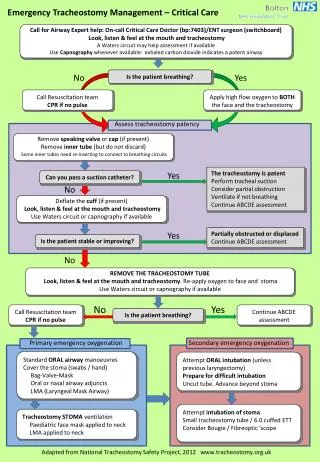
Emergency Interventions 1. Respiratory Distress?? a. Attempt to suction trach b. Attempt to ventilate trach with ambu bag c. Change trach if suctioning/ ventilation unsuccessful 2. No Spontaneous Respirations/Cardiopulmonary arrest?? a. Press Code Button B. Attempt to ventilate with ambu bag c. If ventialtion unsuccessful, suction trach tube. If patient remains obstructed, perform emergency trach change. 3. Critical Care: Accidental decannulation with stay sutures still intact?? A. Call for help B. Lift stay sutures off chest and maintain a gentle pulling pressure upward C. Insert Same Size trach tube
Benefits: Silicone remains soft and flexible in the trachea Can be used for 3 months, as with all Bivonatrachs Kink resistant Atraumatic, contoured neck flange (causing less device related pressure directly to the neck). Recommended for some of the NICU patients having chubby neck s or short necks. Disadvantages: Tube is composed partially of metal, therefore, needs to be changed out prior to going to MRI. Substitute with a non-metal Bivona (same size) or a Shiley equivalent for the scan. BIVONA FLEXTEND TRACH TUBES
Cuffed Bivona Tracheostomy Tubes ‘ BivonaFome-Cuf Trach Tube Tight To Shaft (TTS) Cuffed Trach Tube
Bivona Tracheostomy Tubes Hyper-Flex Bivona Tracheosotmy Tube Bivona Un-Cuffed Tube
Trachesotomy Care 1. Trach care is to be done with cluster cares every 3-4hours. Spray the tips of the Q-Tips with Wound Cleanser and clean around the stoma and underneath the trach ties. Assess superior and inferior aspects of the stoma site. Replace Replicare Thin if loose. Use Exudry if patient has excessive secretions noted peri-stoma. This will help to wick away the moisture. Do not tuck guaze sponges under the trach tu as this may displace the trach tube. 2. Trach ties are changed q day and prn if soiled or damp. Cleanse & assess the neck for any skin breakdown. If neck red or excoriated, apply Replicare to back of neck, before applying new Velcro ties. *Treat Skin Irritations/Redness using Protective Measures:A. For minimal irritation (pink skin and irritated), keep area clean & dry, apply treatment as ordered by NNP/MD.B. For moderate irritation (red, excoriated skin) Cleanse area well with Wound Cleanser, pat dry, & apply Replicare Thin.C. For significant irritation (full skin breakdown), apply a small piece of Algisite dressing directly inferior & superior at trach stoma & secure with Replicare Thin. Change Algisite M when it becomes gel-like.
A Few Additional Items to Always Have Handy at the Bedside…… 1. Wedge Popper 2.Obtruarator 3. Neck Roll 4. Twill Tie
Customized Tracheostomy Tubes??? If the Tracheostomy Tube is Customized to CNMC or Customized to the Patient. it will have a special yellow/green label. It will state ‘CUSTOMIZED.’ Keep this Label in the ‘Ready-To-Go’ Bag. Label with patients label & dated as to when it was opened. • Tracheostomy tubes may be a standard size but or customized to meet patient needs. If a customized tracheostomy tube is deemed necessary it may take up to one week to receive. It is always important not to lose this label as this is helpful in the re-ordering process. There are some CNMC customized tracheostomy trach tubes in-house (kept in Trach Pyxis in the OR), but are limited in availability. It is important not to throw out the tracheostomy tubes. Bivonas are to be sent to SPD & the Shiley trachs are to be cleansed at the bedside. If you are in need of a CNMC customized trach please notify J. Amling, P Allen, or your charge nurse.
This sheet is a part of the Tracheostomy Nursing Practice Guidelines. _________ Record suction length on the patient’s “I Have a Tracheostomy” sign at the bedside. Update as trach size changes. __________ Bivona Flextend: Add an additional 2cms on top of the standard sx length quoted on the Insertion Guide Insertion Guide for Suction Catheters
I-View / ICU Ongoing Assessment / Tracheostomy • Document q shift & prn with cares • Do Powerchart Documentation
Stage III Pressure Ulcer NEVER EVENT
What went wrong here? Tracheostomy ties must never be too tight. One should be able to slide only one index finger up under the trach tie at any given time. Also keep in mind, if Velcro ties are too loose, the trach can easily fall out or can move about the trachea which may cause tissue erosion peri-stoma & or within the trachea itself. _______ Tissue erosion from tracheostomy ties cutting into skin
What can we do to prevent skin breakdown around the tracheostomy site?? There needs to be special attention given to the skin condition at the neck , as well as the inferior and superior aspects of the trach stoma. Assessment of stoma needs to be made with each patient cares & tie changes What are Granulomas? An overgrowth of inflammatory tissue, which is caused by tissue irritation from the tracheostomy tube or infection. Some granulomas become so enlarged that it may be difficult to pass a trach tube through the stoma. . Device Related Skin Excoriation & Granulomas Peri-Trach Stoma
Bivona Tracheostomy Tubes 1.Rinse tracheostomy tube under water as to dislodge any mucous from the trach.. 2. Place trach tube in a clear bag along with 2 patient stickers. 3. Nursing must take to SPD as soon as possible. SPD is located in the back of Central Supply. 4. Complete the sigh in sheet at desk & physically hand the bag over to an SPD employee. 5. SPD’s turn-around from drop off to pickup is 2-3hours. Make certain it is picked up within that time frame. You will need to sign the trach out when picking up. This particular trachtuve is most likely your only same size trachestomy tube. It is the responsibility of each nurse to have all supplies in the Ready-to-Go bag. It should be checked at the beginning of each shift.
1.Rinse ‘Shiley’ trach tube under running water. 2. Cleanse at bedside with ½ strength Hydrogen peroxide. 3.Rinse well w/ sterile NS . 4. Air dry on paper towel. 5.Place in sterile container. 6.Label w/ pt’s name , type of trach tube, date original package opened, & dates cleansed. __________________ No peroxide if Shiley tube is cuffed, use only sterile saline as peroxide is destructive to the cuff. May be used for 29 days before discarding. Label container accordingly . Change q Monday & prn Cleansing the‘Shiley’ TracheostomyTube for re-use at the bedside
It is Everyone’s Responsibility to Provide Tracheostomy Education to Families *Document Any & All Tracheostomy Parent Teaching in AD Hoc under Patient/Family Education. There is a Designated area specific for Tracheostomy Education. Take opportunities to educate when Parents visit. Involve them in trach tie changes, Suctioning, Monday trach change scheudle, etc.
References • CNMC Nursing Practice Guidelines 7/2009 “Tracheostomy Management” • Tracheostomy Care Handbook: A Guide for the Healthcare Provider - Portex, Inc./ Product Literature • Pediatric Tracheostomy Care Handbook: An instructional Booklet for Home Care of your Child with a Tracheostomy/ Portex IncProduct Literature ‘Christmas in the BPD Ward’ Photo from the Life of Chevalier Jackson, An Autobiography (Slide 1) • Shiley (2009) “Tracheostomy Tube Home Care Guide” • Bivona (2009) www.smith-medical.com/catalog/ bivona-tracheostomy-tubes/neonatal