Download
1 / 76
800 likes | 1.5k Views
Diagnosis and Treatment of Hepatocellular carcinoma. 萬芳醫院 消化內科 粟發滿 醫師. Epidemiology of Hepatocelluar carcinoma. Estimates from the year 2000 indicate that liver cancer remains the fifth most common malignancy in men and the eighth in women worldwide.

E N D
Diagnosis and Treatment of Hepatocellular carcinoma 萬芳醫院 消化內科 粟發滿 醫師
Epidemiology of Hepatocelluar carcinoma • Estimates from the year 2000 indicate that liver cancer remains the fifth most common malignancy in men and the eighth in women worldwide. • The number of new cases is estimated to be 564,000 per year, including 398,000 in men and 166,000 in women, and it accounts for 6% of all malignancies . • Rates of liver cancer in men are typically 2 to 4 times higher than in women. • The attributable risk estimates for the combined effects of HBV or HCV infections account for well over 80% of liver cancer cases worldwide
Worldwild Incidence and Trends of HCC Bosch et al. Gastroenterology 2004
Worldwild Incidence and Trends of HCC Bosch et al. Gastroenterology 2004
臺 灣 地 區 主 要 癌 症 死 亡 率 趨 勢 圖 每十萬人口 死亡數 45 40 35 30 25 肝癌 20 肺癌 結腸直腸癌 15 10 胃癌 5 口腔癌 ( ) 含口咽及下咽 0 73 74 75 76 77 78 79 80 81 82 83 84 85 86 87 88 89 90 91 92 93 年
Risk factors of HCC Cirrhosis Hepatitis B virus infection Hepatitis C virus infection Genetic Hemochromatosis Congenital Metabolic Disease Gylcogen storage disease type I 1-Antitrypsin deficiency Hereditary tyrosinemia Porphyria Toxin Alcohol Aflatoxin B
Risk factors for HCC worldwide Llovet et al. Lancet 32003
Differences in Age, Sex and Viral Etiology In Taiwanese HCC patients Lu et al. Int J Cancer 2006
台南地區肝細胞癌患者之病因分析 李 川 J Intern Med Taiwan 2003
Odd Ratio of HCC in Subjects Stratified Jointly by HBV and HCV Donato et al. Int J Cancer 1998
Hepatollular carcinoma in alcohol related Cirrhosis patients
Modeling of Odd Ratio of HCC by levels of daily alcohol intake in men and women Donato et al. Am J epidemiol 2002
Odd Ratio of HCC in Men Stratified by Prediagnostic Aflatoxin Exposure Status and HBV Qian et al Cancer Epidemiol Biomarkers Rev 1994
Odd Ratio of HCC Stratified by Hepatic Levels of 4-Aminobiphenyl DNA Adducts and HBV Wang et al Am J epidemiol 1998
Relative risks of liver cancer associated with coffee consumption (per 2 cups/day) Larsson SC. Gastroenterology 2007
Clinical Manifestations of Symptomatic Hepatocellular Carcinoma
Diagnostic criteria for HCC • Cyto-histology criteria • Non-invasive criteria (restricted to cirrhotic patients) 1. Radiological criteria: two coincident imaging techniques Focal lesion > 2 cm with arterial hypervascularization 2. Combined criteria: one imaging technique associated with AFP Focal lesion >2 cm with arterial hypervascularization AFP levels >400 ng/ml
Tumor Markers of HCC Alpha-Fetoprotein -fetoprotein mRNA Lectin reactive -fetoprotein Des--carboxy prothrombin (DCP) (Protein Induced by Vitamin K absence or antagonist II; PIVKA-II) p53 Autoantibodies Transforming Growth Factor-1
Sensitivity, Specificity, Negative Predictive Value, and Positive Predictive Value of AFP for HCC Daniele et al. Gastroenterology 2004
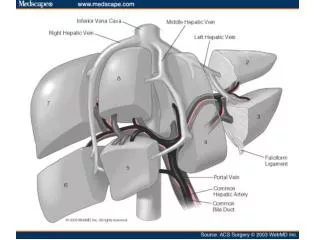
Imaging diagnosis of HCC • Ultrasound • Best diagnostic imaging technique • Capable of detecting tumor >1 cm • Has been useful in serially following cases of cirrhosis to identify hepatocellular cancer when <2 cm and curable • CT scan • Valuable in determining extrahepatic spread of the disease • MRI: Helpful in delineating the details of tumor and the invasion of vessels • Hepatic arteriography • Mostly done to see the anatomy of hepatic vessels and extent of tumor while considering resection, embolization, dearterialization, or intra-arterial infusion of cytotoxic agents • Most useful in detecting angiosarcoma, separating benign versus malignant • Lipoidal angiography and CT • Lipoid is readily taken up by tumor cells • Technique can detect even millimeter-sized lesions
The right lobe HCC with tumour thrombus in the main portal vein
dilated, tortuous and displaced arterial tumour feeders neovasculatures showing a chaotic and disorganized pattern Vascular lakes are present. Angiography of HCC
HCC with portal vein thrombosis on the portal venous phase of hepatic angiogram.
TNM Classification for Hepatocellular Carcinoma, 2002 AJCC Cancer staging 2002
Definitions in the Okuda Staging System Okuda K et al. Cancer 1985
Definitions Used in the Cancer of the Liver Italian Program (CLIP) CLIP group Hepatology 1998
Median Survivals (months) for theThree Prognostic Systems CLIP group Hepatology 1998
Treatment strategies for hepatocellular carcinoma based on tumor stage and Child-Pugh class
Strategy for staging and treatment assignment of HCC according to the BCLC proposal
Strategy for staging and treatment assignment of HCC according to the BCLC proposal
Milan Criteria for Transplantation of the liver • One nodule 2.0–5.0 cm; 2 to 3 nodules all ≤3.0 cm • No gross intrahepatic portal or hepatic vein involvement on imaging • No lymph node or distant metastasis or extrahepatic portal or hepatic vein involvement Mazzaferro et al, NEJM 1996
Liver Transplantation for HCC: Outcomes Applying Milan Criteria Myron Schwartz Gastroenterology 2004
Strategy for staging and treatment assignment of HCC according to the BCLC proposal
Rational for local ablative therapy for liver tumor • It does not have the disadvantage of loss of or limited damage to non-neoplastic parenchyma • It is low-risk procedures • It can be easily repeated when new lesions appear • The low cost, easy availability of the necessary material, and the simple techniques
Percuatneous local ablative therapy of liver tumor • Percutaneous local ablative therapy is indicated for patients with small HCC (<5 cm) confined to the liver that is unresectable due to limited liver reserve or compromised liver function • It is contraindicated in patients with gross ascites, coagulopathy that cannot be corrected, and obstructive jaundice due to the potential risk of bleeding and bile peritonitis.
Local ablative therapy for liver tumor • Percutaneous ethnaol injection therapy (PEIT) • Percutaneous acetic acid injection (PAI) • Radiofrequency ablation (RFA)