Download
1 / 34
340 likes | 391 Views
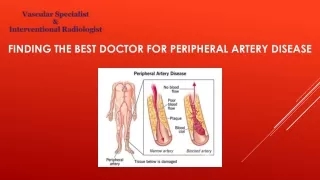
Learn about diagnostic methods, symptoms, and treatments for peripheral artery diseases (PAD) affecting limbs. Understand PAD prevalence, risk factors, classification, and treatment options including revascularization and lifestyle changes.

E N D
Peripheralarterydiseases Jakub Honěk Kardiologická klinika 2.LF UK a FN Motol
Diagnostic methods • Peripheral artery diseases (limb ischemia) • Chronic PAD • Acute limb ischemia • Compressive syndromes • Vasospastic disorders • Specific localization of PAD • Vasculitis
Diagnosticmethods • Medical history, physical examination • Measurement of peripheral arterial pressure (+ ABI, TBI) at rest, after exercise • Plethysmographic examination • TcpO2 • Teadmill walking test • Color duplex sonography • X-ray based methods - DSA, CTA, MRA
Peripheral BP (mmHg)ankle >100…, 50-100 … (claudication), <50 … (criticalischemia)toe < 30 … (criticalischemia)
tcpO2 • Testing peripheral skin perfusion on the capillary level; testing skin nutrition • Closely corresponds to the capillary pressure of O2 →To determine the degree of perfusion (ischemia),evaluate the effectiveness of revascularization,determineamputation line,predict effectofhyperbaric oxygen therapy
tcpO2 (transkutánní měření parciálního tlaku kyslíku ve tkáni)
Plethysmography • Photopletysmography- emitted infrared light is reflected Hb, while in tissues without Hb is absorbed or released (decay curve) →detection of acral blood circulation disorders; examinationpatientswith DM (mediocalcinosis); dif.dg. TOS; cooling test
Duplex ultrasound Bifurcation Atherosclerotic plaque
Peripheralarterydiseases (PAD) • Peripheral artery disease (PAD) generally refers to a disorder that obstructs the blood supply to the lower or upper extremities • 90-95 % atherosclerosis • 5-10% thrombosis, embolism, vasculitis, fibromuscular dysplasia, entrapment • Impcacton qualityoflife + mortality (cardiovascular) • > 50% patients with PAD at the same time suffer from coronary atherosclerosis, 15-40% and carotid atherosclerosis
Modifiable risk factors(atherosclerosis) • Cigarette smoking • Dyslipidemia • Diabetes • Arterial hypertension
Less frequent causes of PAD • Coarctationofthe aorta • Vasculitides • Tromboangiitisobliterans (Buergersdisease) • Peripheralembolisationfromvariousorigins • Entrapmentsy AP • Cysticadventitialdegeneration AP • fibromusculardysplasia • Iliacarteryendofibrosisofcyclists • Primaryvasculartumors • Compression (tumorsetc.) • Vascular trauma • Iatrogenic vascular disease (percutaneous and surgical procedures) • Irradiationarterialdisease
Symptoms • Chronic disease • Claudication – muscle ischemia • Site of stenosis correlates with site of pain • intermittent claudication – on exertion • Critical limb ischemia • Acute vs. chronic • Limb/life threatening disease • paresthesia, pain at rest
Rutheford Peripheralarterialdisease - classification Fontain
Intermittentclaudication • Metabolic demands of muscle not met during exercise • Higher demand (muscle work) • Flow limitation (pressure gradient) • Impaired vasomotion • Steal syndrome • Pain one level bellow stenosis • Tredmill test – determines walking capacity, ABI after exercise (pain + 25% decrease in ABI confirms diagnosis)
Acute limb ischemia • ←70-80% embolicclosure (sudden PAD) • ←30-20% thrombotic occlusion (mostlythrombus on rupturedplaque - acute worsening of existing PAD) • Clinicalpicture- incomplete X completeischemicsy (6Ps) Pain Paleness Pulselessness Paresthesias Paralysis Prostration
Treatmentofacute limb ischemia • i.v. Heparin, i.v. analgesics → urgent revascularization (DSA) • Surgical embolectomy- pelvic arteries, arm and forearm arteries • Endovascular therapy- LTL, thrombus aspiration, mechanical revascularization • Combination of both
Treatmentofchronic PAD • Cardiovascular mortality prevention • antiplatelet drugs (ASA) • risk factor modification (statins!, antihypertensives…) • Lifestyle changes, exercise • QoL improvement – control of claudications • Vasocative agents (cilostazol 2x100 mg, naftidrofuryl 3x200 mg) • Few clinical data supporting effectivity of vasoactive drugs • Prostanoids – critical limb ischemia • Exercise • Revascularization
Treatmentofchronic PAD • Methods of revascularization • Endovascular (percutaneous, invasive) • PTA (DEB; BMS, DES); stentgrafts; SIR; thrombolysis • surgery • bypass, endarterectomy, amputation • Stimulation of angiogenesis(stem cells) ?? • Lumbar sympathectomy
Lerich`s syndrome(total subrenal occlusion of aorta) • Claudication in buttocks, hypotrophy of thighs, impotence in ♂ • Treatment - aorto-bifemoral bypass
Compressivesyndromes • compressionof arteries, veins, nerves (or all 3 systems) – - anatomical structures (costoclavicular sy) - anatomical anomalies (cervical rib) - different course (medial course of a.poplitea)
Thoracicoutlet syndrome • compression of neurovascular bundle • between scalenous muscles • In costoclavicular space • at the insertion of m. pectoralis minor
Thoracicoutlet syndrome • symptomatology - neurogenic 95% - arterial 3-5% - venous 2% • symptoms-carrying an umbrella, washing windows, painting walls, driving… • Therapy - rehabilitation→ improvements up to 70% within a few months - surgical(resection of the first rib) in severe disability
Costoclavicular syndrome • represents 80% of all TOS • compression of neurovascular bundle (a.,v., n.) between the clavicle and the first rib
Entrapment syndrome ofpoplitealartery • the most common cause of limb ischemia in patients under 35 years • ← abnormal course of PA • ← non-physiological hypertrophy of the surrounding structures • ← presence of abnormal structures (fibrous bands) dg. MR- relation of vascular bundle with the surrounding muscle or connective structures th. surgery (LTL and PTA only to improve the outflow tract for surgical reconstruction)
Specificlocalizationof PAD • Visceral ischemia • Carotid artery disease • Renal arteries
Vasospasticdisorders • Usually reversible localized narrowing of smallarteries • primary disorders do not lead to trophic changes • Raynaudsphenomenon • Primary: morbusRaynaud- etiology is not clearly known, suspected failure of regulation at the level of the terminal vascular bed • Secondary: Raynaud´ssyndrome – secondary to another underlying disease
Raynaud's phenomenon • 1st phase: ischemia → morbidly pale fingers, paresthesia, 5-60 min. • 2nd phase:stasis of blood in the capillaries and veins → cyanosis • 3rd phase: reactive hyperemia → reddening
PrimaryRaynaud's syndrome • paroxysmal character, symmetrically, except thumb • women 5x more often than men • ♀ between puberty and 30 years old, after pregnancy or menopause problems often disappear
SecondaryRaynaud'ssyndrome • Connective tissue disorders • SLE, RA, sclerodermia… • PAD • Buergers disease, atherosclerosis, TOS… • Drugs • Occupational diseases • Vibration – drilling, cold exposure • Malignancy • Other causes
Takehomemessages • PAD – occlusive diseases of peripheral (limb) arteries • 90% atherosclerosis (modfiable risk factors – smoking!, CV mortality) • Imaging – DUS, CT (MR), angiography • Chronic PAD (claudication, crtitical limb ischemia) vs. Acute limb ischemia • Treatment – CV risk modification + revascularization (endovascular, surgical) • Many other disorders (vasculitides, compression sy., vasospastic disorders…)