Download
1 / 13
130 likes | 255 Views
Collaborating to Put Evidence-based Asthma Care Into Action. James P. Kiley, M.S., Ph.D. Director Division of Lung Diseases National Capital Region Asthma Partnership Conference May 6, 2010. Burden of Asthma. Lost productivity 11 million work days lost per year

E N D
Collaborating to Put Evidence-based Asthma Care Into Action James P. Kiley, M.S., Ph.D. Director Division of Lung Diseases National Capital Region Asthma Partnership Conference May 6, 2010
Burden of Asthma • Lost productivity • 11 million work days lost per year • 14 million school days lost per year (21% children w. asthma miss >2 weeks) • 50% of national survey sample missed >6 days in one year • Reduced quality of life • >10% of people with asthma restrict activities • 48% parents in national survey have children avoid exertion • 30% don’t sleep through the night • High morbidity • 484,000 hospitalizations, all ages • Most common reason for hospitalization in children • High cost • $20.7 billion annual direct & indirect costs (projected 2010) • Death • 3,365 deaths in 2006
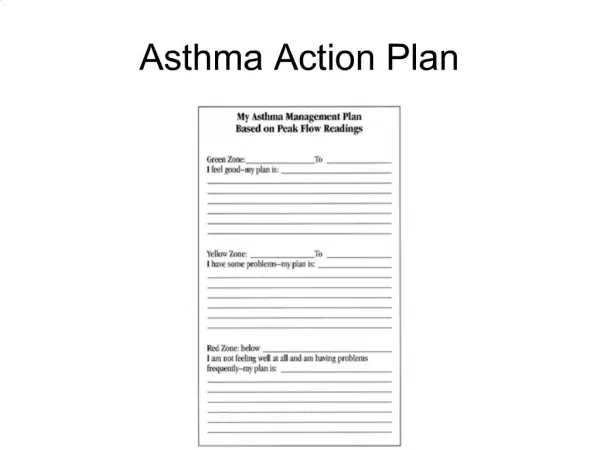
NAEPP EPR-3 Guidelines Implementation Panel (GIP) 2008 Prioritized 6 key messages from evidence based EPR-3 • Inhaled steroids are most effective for long term control All patients should receive: • Written Action Plan • Initial assessment of severity • Follow up assessment of control • Regular “asthma check ups” • Assessment and advice about environmental exposures
Discrepancy Between Promise of Control and Reality From numerous studies: • Physicians prescribe inhaled corticosteroids inappropriately: e.g., one study showed only 30% of patients with persistent asthma were on inhaled corticosteroids. From recent nationwide survey of adults with asthma*: • Patients do not use medications appropriately: • 42% reported they intermittently stop taking ICS • Patients do not appreciate that Asthma Can Be Controlled • 70% said their asthma was “in control” BUT 47% of them actually had poorly controlled asthma. • 16% reported use of quick-relief inhaler every day • 29% reported fear of asthma attacks keep them from doing the things they want *Asthma Insight and Management Survey; Medical News Today, Nov. 2009 (national sample; sponsored by Schering and Merck)
What Can Make the Promise Real? • Understanding and believing that ASTHMA CAN BE CONTROLLED • Adherence, Adherence, Adherence
Factors Influencing Patient Adherence Patient-providercommunication is a partnership Adherence Phenotype External Supports are in place - Social/family - Access to care - Reinforcement Treatment Regimen: - Fits into daily routine - Can discuss & overcome fears/barriers Patient Characteristics - Expects treatment to work - Has self-management skills - Has belief in self-efficacy
Factors Influencing Physician Adherence Expects guidelines will work Has skills & self efficacy Adherence Phenotype Can overcome inertia of previous practice routines Is familiar with guidelines External Supports are in Place - Time - Reimbursement - Space & Equipment - Patient education materials
Factors to Promote Adherence • Involve different groups and improve communication among them: • Patients and public ■ Policy makers • Healthcare providers ■ Health Systems • Schools and community groups • Foster systems integration • Create tools for patients and providers
National Asthma Control Initiative (NACI) • NACI, launched by NAEPP, puts the EPR-3 priority messages and strategies in motion nationwide through partnership activities
NACI Commitments to National Capitol Region • Children’s Research Institute at Children’s National Medical Center in DC: will pilot electronic Asthma Encounter Form to transition patients from ED to Primary Care • Allergy and Asthma Network: will pilot self-paced asthma education for patients and families • Medical Society of Virginia Foundation: will create a maintenance of certification asthma education module for physicians • National Respiratory Training Center: will conduct continuing medical education program for physicians and allied health professionals • National Environmental Education Foundation in DC: will train medical school faculty, students, and residents to use key messages with focus on environmental management
NACI • Keep in touch with NACI: to start, sign up for In the Know e-Newsletter. • NACI congratulates National Capital Region Asthma Partnership initiatives. • Your collaborative projects will improve patient and provider adherence to strategies that will realize the promise of Asthma Control.
Research, Guidelines & Clinical PracticeA Dynamic Interaction • Clinical Practice Communities • Implement Guidelines in clinic and community settings • Share lessons learned • Identify clinical controversies • Observe variations in responsiveness • Help define research questions & priorities • NACI support • Guidelines • Provide recommendations for clinical practice • Identify gaps in evidence • Clinical Research • Investigate issues of clinical concern • Study results provide evidence for updating guidelines
Judith Taylor-Fishwick, MSc, AE-C Director (USA Office)National Respiratory Training Center Suffolk, Virginia